Vous aimerez peut-être aussi
- Documentation ExamplesDocument5 pagesDocumentation ExamplesErika HarveryPas encore d'évaluation
- Grammar Workbook Gr. 4 - HomeschoolDocument195 pagesGrammar Workbook Gr. 4 - HomeschoolJessica Pollard Adams100% (2)
- The Cell: Transport Mechanisms and Cell Permeability: Physioex 1Document28 pagesThe Cell: Transport Mechanisms and Cell Permeability: Physioex 1mdarln808Pas encore d'évaluation
- Doh Health Programs MaternalDocument82 pagesDoh Health Programs MaternalWilma Nierva BeraldePas encore d'évaluation
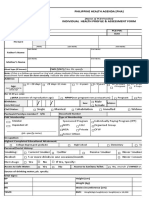
- PHA Individual Health Profile & Assessment Form As of Oct.09, 2017Document8 pagesPHA Individual Health Profile & Assessment Form As of Oct.09, 2017Eden VblagasyPas encore d'évaluation
- Advanced Trauma Life SupportDocument8 pagesAdvanced Trauma Life SupportAbouzr Mohammed ElsaidPas encore d'évaluation
- Essential Newborn Care: The DOH/WHO ProtocolDocument21 pagesEssential Newborn Care: The DOH/WHO ProtocolfelicitycherubPas encore d'évaluation
- Ao 2016-0035Document9 pagesAo 2016-0035Donna Miranda100% (5)
- GRADE IV Science QuizDocument2 pagesGRADE IV Science QuizRhea Somollo Bolatin100% (3)
- Family Structure, Characteristics and DynamicsDocument6 pagesFamily Structure, Characteristics and DynamicsErilyn Leigh ManaloPas encore d'évaluation
- FHSIS Form TCL Pre NatalDocument11 pagesFHSIS Form TCL Pre NatalEden Vblagasy100% (5)
- FHSIS Form TCL Pre NatalDocument11 pagesFHSIS Form TCL Pre NatalEden Vblagasy100% (5)
- The Nervous System: The Central Processing UnitDocument85 pagesThe Nervous System: The Central Processing UnitGeoffrey MilesPas encore d'évaluation
- Buntis CongressDocument3 pagesBuntis CongressSaraJaneOmandamPas encore d'évaluation
- Target Client List For Nutrition and Expanded Program For ImmunizationDocument7 pagesTarget Client List For Nutrition and Expanded Program For ImmunizationEden Vblagasy0% (1)
- Target Client List For Nutrition and Expanded Program For ImmunizationDocument7 pagesTarget Client List For Nutrition and Expanded Program For ImmunizationEden Vblagasy0% (1)
- Mothers ClassDocument73 pagesMothers ClassJuliana Andres83% (6)
- BHW Monthly Report FormDocument3 pagesBHW Monthly Report FormPearlCarylCatantan-Cadavis80% (5)
- Child TCLDocument28 pagesChild TCLNandie JoyPas encore d'évaluation
- AO 2009 0025 Essential Newborn CareDocument15 pagesAO 2009 0025 Essential Newborn Carejulesubayubay542895% (21)
- Garantisadong PambataDocument3 pagesGarantisadong Pambataboss062212Pas encore d'évaluation
- Implementing Guidelines For The Establishment of HPN and DM ClubDocument15 pagesImplementing Guidelines For The Establishment of HPN and DM ClubChristian Felix Ignacio100% (1)
- Family Planning New Couples Profile FormDocument2 pagesFamily Planning New Couples Profile FormEden VblagasyPas encore d'évaluation
- Bag Technique and The PHN BagDocument4 pagesBag Technique and The PHN BagkirbyroohPas encore d'évaluation
- FPCBT Level 1 For FacilitatorsDocument519 pagesFPCBT Level 1 For FacilitatorsMichael Villavert100% (1)
- Advisory 3 With Amendment - MR OPV SIADocument1 pageAdvisory 3 With Amendment - MR OPV SIAD Alfz EinsTein JDPas encore d'évaluation
- B C P C: ActionplanDocument5 pagesB C P C: ActionplanMicky MorantePas encore d'évaluation
- Narrative Report ShadowingDocument18 pagesNarrative Report ShadowingThriska Ravven Resurreccion100% (1)
- Mothers ClassDocument3 pagesMothers ClassGerald Resubal Oriña100% (1)
- Mother and Child Protection Card (MCP Card)Document40 pagesMother and Child Protection Card (MCP Card)Venkat67% (3)
- Id No.: CVD/NCD Assessment Form For Adults 20 Years Old and AboveDocument1 pageId No.: CVD/NCD Assessment Form For Adults 20 Years Old and AboveNel Jerez67% (3)
- NEW m1m2 Reporting FormDocument24 pagesNEW m1m2 Reporting FormDeyeck Verga100% (8)
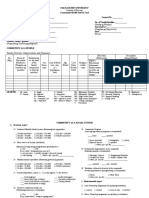
- CHN Community Survey FormDocument2 pagesCHN Community Survey FormRamyaj Odagor100% (1)
- DOH Pregnancy Tracking FormDocument9 pagesDOH Pregnancy Tracking FormEden VblagasyPas encore d'évaluation
- Health History Taking FormDocument4 pagesHealth History Taking FormKeana Dacayana100% (1)
- Current Clinical Strategies, Pediatric History and Physical ExaminationDocument96 pagesCurrent Clinical Strategies, Pediatric History and Physical ExaminationMocanu Cristina-Viorica100% (1)
- MNCHN MopDocument68 pagesMNCHN Mopmbs_md100% (1)
- PRU LIFE UK - Product SummaryDocument36 pagesPRU LIFE UK - Product SummaryEden VblagasyPas encore d'évaluation
- Birthing Facility IPCR RM Ver 1Document4 pagesBirthing Facility IPCR RM Ver 1RvBombeta50% (2)
- BHW Summary of Services Reporting Form 1Document5 pagesBHW Summary of Services Reporting Form 1MOLINO II SOCIAL SERVICESPas encore d'évaluation
- Acid Base AnswersDocument4 pagesAcid Base Answersapi-232466940Pas encore d'évaluation
- Garantisadong PambataDocument5 pagesGarantisadong PambataRolena Johnette B. PiñeroPas encore d'évaluation
- Answers To The Cambridge Checkpoint Science 2Document28 pagesAnswers To The Cambridge Checkpoint Science 2Nur Dina ZaulkifleePas encore d'évaluation
- Oral ExamDocument4 pagesOral ExamOdonchimeg ElbegzayaPas encore d'évaluation
- HPN-DM Draft ResolutionDocument4 pagesHPN-DM Draft ResolutionRoselle Lim100% (2)
- MBFHI Self-Assessment ToolDocument64 pagesMBFHI Self-Assessment ToolMash JumahariPas encore d'évaluation
- BHB Orientation For NDPs-1Document19 pagesBHB Orientation For NDPs-1Shevan Simon AliñabonPas encore d'évaluation
- Module 3Document2 pagesModule 3Rodeza Abella100% (2)
- HBMR 2Document1 pageHBMR 2Borbe ClauPas encore d'évaluation
- Accomplishment Report Human Resource For Health (HRH) Deployment Program For The Month of - , 2021Document4 pagesAccomplishment Report Human Resource For Health (HRH) Deployment Program For The Month of - , 2021Ace Gaming100% (1)
- Scale For Ranking Health Conditions and Problems in Family Nursing PracticeDocument3 pagesScale For Ranking Health Conditions and Problems in Family Nursing PracticeDjan Kurvie Valencerina100% (1)
- Glanders in HorseDocument43 pagesGlanders in HorseWerner AlbuquerquePas encore d'évaluation
- DOH Programs A-Z PhilippinesDocument1 pageDOH Programs A-Z PhilippinesDianne Macaraig100% (4)
- PIMAMDocument20 pagesPIMAMRoger Chiu100% (3)
- Copar Process ModuleDocument5 pagesCopar Process ModuleeldigertPas encore d'évaluation
- Family Planning Client Assessment FormDocument3 pagesFamily Planning Client Assessment FormGeline Joy D. Samillano100% (2)
- Nurse Deployment Program NDP Examination NotesDocument44 pagesNurse Deployment Program NDP Examination NotesAngelo Quixote100% (1)
- Post Partum AssessmentDocument3 pagesPost Partum Assessmentdanica grace gubaPas encore d'évaluation
- Family Planning Service Record Form IDocument4 pagesFamily Planning Service Record Form IBarangay Lam-anPas encore d'évaluation
- dm2021 0261 Advisory On Provisional Primary Care CertificationDocument2 pagesdm2021 0261 Advisory On Provisional Primary Care CertificationJessa Mae75% (4)
- FP Form1 V3.0 2016Document3 pagesFP Form1 V3.0 2016Lorenz Joey Ricarte100% (2)
- The Doh Nutrition ProgramDocument10 pagesThe Doh Nutrition ProgramDianne MaePas encore d'évaluation
- Module 7Document15 pagesModule 7Alilem RhuPas encore d'évaluation
- Action Plan Edited2Document3 pagesAction Plan Edited2Ardee Marius GuzmanPas encore d'évaluation
- Field Health Services and Information System 1Document8 pagesField Health Services and Information System 1Vhince PiscoPas encore d'évaluation
- GI Practice Exam With AnswersDocument3 pagesGI Practice Exam With AnswerskcpuffsPas encore d'évaluation
- Nurse Deployment Program (NDP) Examination NotesDocument44 pagesNurse Deployment Program (NDP) Examination Notesdeeday echavez93% (27)
- Unang Yakap: Essential Newborn Care (ENC) ProtocolDocument13 pagesUnang Yakap: Essential Newborn Care (ENC) ProtocolJan Oliver YaresPas encore d'évaluation
- Prenatal Record FormDocument3 pagesPrenatal Record FormIZABELLA BEATRICE ABANOPas encore d'évaluation
- Bcongress 2016Document2 pagesBcongress 2016Christian RiveraPas encore d'évaluation
- Garantisadong PambataDocument3 pagesGarantisadong PambataJieann Crissel PilapilPas encore d'évaluation
- Inadequate Living Space - NCPDocument2 pagesInadequate Living Space - NCPissaiahnicollePas encore d'évaluation
- My O&g Clerking TemplateDocument8 pagesMy O&g Clerking TemplateFarah FadzilPas encore d'évaluation
- Maternal & Child Health BookletDocument17 pagesMaternal & Child Health BookletAtina LavadiaPas encore d'évaluation
- ErlinaDocument5 pagesErlinaCharles Vergel Sabaldan MarceraPas encore d'évaluation
- Dermatology History and Examination FormDocument4 pagesDermatology History and Examination FormЂорђеPas encore d'évaluation
- Discharge Plan FormatDocument3 pagesDischarge Plan FormatYuraPas encore d'évaluation
- Print NCLEX Study - Mark Klimek Blue BookDocument17 pagesPrint NCLEX Study - Mark Klimek Blue Booklento1990Pas encore d'évaluation
- MARCH 2017 NDP Accomplishment Report Sulat Eastern SamarDocument21 pagesMARCH 2017 NDP Accomplishment Report Sulat Eastern SamarEden VblagasyPas encore d'évaluation
- JUNE 2017 NDP Accomplishment ReportDocument20 pagesJUNE 2017 NDP Accomplishment ReportEden VblagasyPas encore d'évaluation
- DOH MNCHN Continuation ReportDocument14 pagesDOH MNCHN Continuation ReportEden VblagasyPas encore d'évaluation
- Summary Report On Pen ImplementationDocument1 pageSummary Report On Pen ImplementationEden VblagasyPas encore d'évaluation
- EASTERN Samar 2017-2021 Projected Population (Based On 2015 Actual Census)Document52 pagesEASTERN Samar 2017-2021 Projected Population (Based On 2015 Actual Census)Eden Vblagasy100% (1)
- Human Reproductive System - Wikipedia PDFDocument4 pagesHuman Reproductive System - Wikipedia PDFAubrey EuropePas encore d'évaluation
- Chicken Infectious AnemiaDocument6 pagesChicken Infectious AnemiaChristian VillarrealPas encore d'évaluation
- V. Diagnostic ExaminationDocument3 pagesV. Diagnostic ExaminationArlene MacatangayPas encore d'évaluation
- GumboroDocument36 pagesGumboroSissi Delgado50% (2)
- BronopolDocument3 pagesBronopolImut MainahPas encore d'évaluation
- D - Rochmanita Safitri (Skoliosis)Document59 pagesD - Rochmanita Safitri (Skoliosis)Siska FriedmanPas encore d'évaluation
- GPMRDocument5 pagesGPMRwisdom hameloPas encore d'évaluation
- Concept Paper Dog SchoolDocument4 pagesConcept Paper Dog SchoolClea Marie Mission100% (2)
- Obstetrics - Anatomy & PhysiologyDocument12 pagesObstetrics - Anatomy & PhysiologyDexter Lendio0% (1)
- Xenogears God and Mind Vol 1: LostDocument72 pagesXenogears God and Mind Vol 1: LostJemjem Veneracion100% (1)
- Maniobras QuirurgicasDocument6 pagesManiobras Quirurgicasyesmaster15100% (3)
- Sharks - WorksheetDocument3 pagesSharks - WorksheetLisaStembelPas encore d'évaluation
- Applied Surgical AnatomyDocument52 pagesApplied Surgical AnatomyEmad AdelPas encore d'évaluation
- Natural Family Planning InstructionsDocument5 pagesNatural Family Planning Instructionsjackie_mePas encore d'évaluation
- Technique - For - The - Collection - of - Clear - Urine in CrocsDocument6 pagesTechnique - For - The - Collection - of - Clear - Urine in CrocsGalo Macias LopezPas encore d'évaluation
- Final Thesis Document 1Document40 pagesFinal Thesis Document 1api-456816629Pas encore d'évaluation
- DMDS MSDSDocument11 pagesDMDS MSDSamirhosseine00Pas encore d'évaluation
- English Exam 2.1Document10 pagesEnglish Exam 2.1John dela CruzPas encore d'évaluation