Vous aimerez peut-être aussi
- Fdocuments - in - Chapter 2 Structural Chapter 2 Structural Modeling Digital System Designs andDocument26 pagesFdocuments - in - Chapter 2 Structural Chapter 2 Structural Modeling Digital System Designs andGuru VelmathiPas encore d'évaluation
- Publication Ethics GuideDocument6 pagesPublication Ethics GuideGuru VelmathiPas encore d'évaluation
- 1 s2.0 S2213138822001102 MainDocument8 pages1 s2.0 S2213138822001102 MainGuru VelmathiPas encore d'évaluation
- Detection of The Fungal Infection in Post-Harvest Onions by An Electronic NoseDocument3 pagesDetection of The Fungal Infection in Post-Harvest Onions by An Electronic NoseGuru VelmathiPas encore d'évaluation
- Focal Cosine Metric and Adaptive Attention Module Improve Siamese CNNs for Scene ClassificationDocument15 pagesFocal Cosine Metric and Adaptive Attention Module Improve Siamese CNNs for Scene ClassificationGuru VelmathiPas encore d'évaluation
- Manual For Research and Publication Ethics in Science and EngineeringDocument174 pagesManual For Research and Publication Ethics in Science and EngineeringGuru VelmathiPas encore d'évaluation
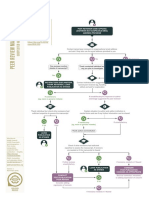
- Peer Review Manipulation After Publication Cope FlowchartDocument1 pagePeer Review Manipulation After Publication Cope FlowchartGuru VelmathiPas encore d'évaluation
- Classifying Analog and Digital Circuits With Machine Learning Techniques Toward Mixed-Signal Design AutomationDocument4 pagesClassifying Analog and Digital Circuits With Machine Learning Techniques Toward Mixed-Signal Design AutomationGuru VelmathiPas encore d'évaluation
- Overlapping PublicationsDocument60 pagesOverlapping PublicationsGuru VelmathiPas encore d'évaluation
- Dokumen - Tips Verilog BasicDocument151 pagesDokumen - Tips Verilog BasicGuru VelmathiPas encore d'évaluation
- A Web-Based Visualization and Animation Platform For Digital Logic DesignDocument15 pagesA Web-Based Visualization and Animation Platform For Digital Logic DesignGuru VelmathiPas encore d'évaluation
- Growing Cosine Unit Activation Function Speeds Up Training and Reduces Parameters in CNNsDocument14 pagesGrowing Cosine Unit Activation Function Speeds Up Training and Reduces Parameters in CNNsGuru VelmathiPas encore d'évaluation
- Logic Synthesis Meets MLDocument23 pagesLogic Synthesis Meets MLGuru VelmathiPas encore d'évaluation
- 4859-Article Text-9057-1-10-20210502Document6 pages4859-Article Text-9057-1-10-20210502Guru VelmathiPas encore d'évaluation
- ML Mentorship Prahitha Movva V1Document5 pagesML Mentorship Prahitha Movva V1Guru VelmathiPas encore d'évaluation
- Top 7 Data Streaming Tools For Real-Time AnalyticsDocument8 pagesTop 7 Data Streaming Tools For Real-Time AnalyticsGuru VelmathiPas encore d'évaluation
- Survey Paper For Activation Functions Bhavya+Document5 pagesSurvey Paper For Activation Functions Bhavya+Guru VelmathiPas encore d'évaluation
- Machine Learning For Electronic Design Automation: A SurveyDocument44 pagesMachine Learning For Electronic Design Automation: A SurveyGuru VelmathiPas encore d'évaluation
- Classifying Breast Cancer Histopathology Images Using Discriminative PatchesDocument16 pagesClassifying Breast Cancer Histopathology Images Using Discriminative PatchesGuru VelmathiPas encore d'évaluation
- Prospects for Analog Circuits in Deep Learning AcceleratorsDocument6 pagesProspects for Analog Circuits in Deep Learning AcceleratorsGuru VelmathiPas encore d'évaluation
- Analog Modeling Using Event-Driven HDLsDocument4 pagesAnalog Modeling Using Event-Driven HDLsGuru VelmathiPas encore d'évaluation
- 2B 1 Jiang HuDocument36 pages2B 1 Jiang HuGuru VelmathiPas encore d'évaluation
- Internet of Things: Kanak Manjari, Madhushi Verma, Gaurav SingalDocument20 pagesInternet of Things: Kanak Manjari, Madhushi Verma, Gaurav SingalCristhian Jover CastroPas encore d'évaluation
- Diabetic Retinopathy Diagnosis Using Multichannel Generative Adversarial Network With SemisupervisionDocument12 pagesDiabetic Retinopathy Diagnosis Using Multichannel Generative Adversarial Network With SemisupervisionGuru VelmathiPas encore d'évaluation
- Image Synthesis in Multi-Contrast MRI With Conditional Generative Adversarial NetworksDocument14 pagesImage Synthesis in Multi-Contrast MRI With Conditional Generative Adversarial NetworksGuru VelmathiPas encore d'évaluation
- Iot Use Cases:: Start Your Connected Journey HereDocument11 pagesIot Use Cases:: Start Your Connected Journey HereAR BushraPas encore d'évaluation
- Synthesis of 3D MRI Brain Images With Shape and Texture Generative Adversarial Deep Neural NetworksDocument14 pagesSynthesis of 3D MRI Brain Images With Shape and Texture Generative Adversarial Deep Neural NetworksGuru VelmathiPas encore d'évaluation
- Value Engineering (Ve) Application in Infrastructure Projects by Public-Private Partnerships (PPPS)Document9 pagesValue Engineering (Ve) Application in Infrastructure Projects by Public-Private Partnerships (PPPS)Guru VelmathiPas encore d'évaluation
- Iot Monetization 0Document11 pagesIot Monetization 0Andrey KuznecovPas encore d'évaluation
- Valueengineering 141206000637 Conversion Gate02 PDFDocument36 pagesValueengineering 141206000637 Conversion Gate02 PDFRachanesh GhatgePas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Balbir PashaDocument23 pagesBalbir PashaEapsita PahariPas encore d'évaluation
- Queer Theory (Mary Klages)Document6 pagesQueer Theory (Mary Klages)Felipe Pimentel100% (1)
- PSYCHOLOGYDocument12 pagesPSYCHOLOGYMichelle GoPas encore d'évaluation
- 09.3 - Cason-FINAL DISSERTATION - CH 1-5 - Clean - 8.19.19 - ASDocument223 pages09.3 - Cason-FINAL DISSERTATION - CH 1-5 - Clean - 8.19.19 - ASeva pandanaPas encore d'évaluation
- Chapleau and Oswald Power Sex and Rape Myth AccetanceDocument14 pagesChapleau and Oswald Power Sex and Rape Myth AccetanceShika ChristianPas encore d'évaluation
- NYU Paper - Not Like A Virgin: Talking About Nonmarital SexDocument13 pagesNYU Paper - Not Like A Virgin: Talking About Nonmarital SexNYU Press94% (17)
- Treating Psychosexual Disorders and ParaphiliasDocument13 pagesTreating Psychosexual Disorders and ParaphiliasOmar IzzoPas encore d'évaluation
- Summary of Anti-Photo and Video Voyeurism Act of 2009 (Republic Act No. 9995, 27 July 2009)Document3 pagesSummary of Anti-Photo and Video Voyeurism Act of 2009 (Republic Act No. 9995, 27 July 2009)Grandeur P. G. GuerreroPas encore d'évaluation
- SRHR - FGD With Young PeopleDocument3 pagesSRHR - FGD With Young PeopleMandira PrakashPas encore d'évaluation
- Leahy, Negotiating StigmaDocument223 pagesLeahy, Negotiating StigmaJohnPas encore d'évaluation
- Sextraficing and Social Media Essay 1Document6 pagesSextraficing and Social Media Essay 1api-477325533Pas encore d'évaluation
- Physical Education and Health Module (Fourth Grading)Document16 pagesPhysical Education and Health Module (Fourth Grading)Dennmark IgutPas encore d'évaluation
- 10 of The Most Popular Destinations For Sex Tourism - TheRichestDocument11 pages10 of The Most Popular Destinations For Sex Tourism - TheRichestMegan Jane JohnsonPas encore d'évaluation
- Brief Sexual Attitudes Scale surveyDocument1 pageBrief Sexual Attitudes Scale surveyDaniela Stoica50% (2)
- ACC102-Chapter1new 000Document13 pagesACC102-Chapter1new 000Ankita T. MoorePas encore d'évaluation
- NOTES ON SEXUAL ADDICTIONDocument50 pagesNOTES ON SEXUAL ADDICTIONnayadampa100% (1)
- SEXUAL DEVIANCY Presentation ReportDocument11 pagesSEXUAL DEVIANCY Presentation ReportHardwee Cadungog Omila100% (1)
- Introduction (Prostitution) - WPS PDF ConvertDocument6 pagesIntroduction (Prostitution) - WPS PDF ConvertCamhyr DelgadoPas encore d'évaluation
- The Porn Circuit - Covenant Eye - DesconocidoDocument47 pagesThe Porn Circuit - Covenant Eye - DesconocidoirvmacPas encore d'évaluation
- Pornography Statistics: 250+ Facts, Quotes, and Statistics About Pornography Use (2013 Edition)Document33 pagesPornography Statistics: 250+ Facts, Quotes, and Statistics About Pornography Use (2013 Edition)Zinc MarquezPas encore d'évaluation
- Offenses Against Sexual Freedom and IntegrityDocument20 pagesOffenses Against Sexual Freedom and IntegrityFelixDelux2023roPas encore d'évaluation
- Imasen Philippine Manufacturing Corporation, Petitioner, vs. Ramonchito T. Alcon and Joann S. PapaDocument3 pagesImasen Philippine Manufacturing Corporation, Petitioner, vs. Ramonchito T. Alcon and Joann S. PapaCharlie MagnePas encore d'évaluation
- Level 7 HfleDocument21 pagesLevel 7 HfleFaustina WigginsPas encore d'évaluation
- Soft Dude Analisis EkstrinsikDocument9 pagesSoft Dude Analisis EkstrinsikImuh A.Pas encore d'évaluation
- Cases On VawcDocument10 pagesCases On VawcjdenilaPas encore d'évaluation
- The Interactionist Approach: Client Individual or Group System Group, Agency, or OtherDocument27 pagesThe Interactionist Approach: Client Individual or Group System Group, Agency, or OtherRonie Bongolo Dacuba0% (1)
- Health Education For Behavior Change - A Workbook To ImproveDocument42 pagesHealth Education For Behavior Change - A Workbook To ImproveNayyar Raza KazmiPas encore d'évaluation
- O'Connell Davidson 2003 Sleeping With The Enemy, Problems With Feminist Abolitionists StanceDocument9 pagesO'Connell Davidson 2003 Sleeping With The Enemy, Problems With Feminist Abolitionists StanceniggrasPas encore d'évaluation
- Module 4: Sexual Self Sexual Self Concept Defined: Gender Gender Identity Gender RoleDocument14 pagesModule 4: Sexual Self Sexual Self Concept Defined: Gender Gender Identity Gender RoleAngel Jasmin TupazPas encore d'évaluation
- The Following Text Is For Questions 1 To 3Document5 pagesThe Following Text Is For Questions 1 To 3Alfi HasanahPas encore d'évaluation