Vous aimerez peut-être aussi
- The Role of Tobacco Growing in Rural LivelihoodsDocument28 pagesThe Role of Tobacco Growing in Rural LivelihoodsIndonesia TobaccoPas encore d'évaluation
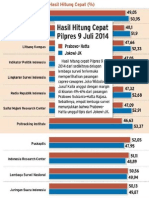
- QuickCount BIDocument1 pageQuickCount BIIndonesia TobaccoPas encore d'évaluation
- SpreadofVote JakartaPostDocument1 pageSpreadofVote JakartaPostIndonesia TobaccoPas encore d'évaluation
- The Role of Tobacco Growing in Rural LivelihoodsDocument28 pagesThe Role of Tobacco Growing in Rural LivelihoodsIndonesia TobaccoPas encore d'évaluation
- Community Partnership ContactsDocument8 pagesCommunity Partnership ContactsIndonesia TobaccoPas encore d'évaluation
- Exposure To Environmental Tobacco Smoke Among South Korean AdultsDocument33 pagesExposure To Environmental Tobacco Smoke Among South Korean AdultsIndonesia TobaccoPas encore d'évaluation
- NCDs Report Summary - WHODocument8 pagesNCDs Report Summary - WHOIndonesia Tobacco100% (1)
- PakistanDocument1 pagePakistanIndonesia TobaccoPas encore d'évaluation
- Source: WHODocument2 pagesSource: WHOIndonesia TobaccoPas encore d'évaluation
- The Industry Menthol ReportDocument250 pagesThe Industry Menthol ReportIndonesia TobaccoPas encore d'évaluation
- Framework Convention On Tobacco Control - FCTC EnglishDocument42 pagesFramework Convention On Tobacco Control - FCTC EnglishIndonesia TobaccoPas encore d'évaluation
- Master Settlement AgreementDocument88 pagesMaster Settlement AgreementIndonesia TobaccoPas encore d'évaluation
- Rules Concerning The Ban On Smoking On European Parliament's PremiseDocument4 pagesRules Concerning The Ban On Smoking On European Parliament's PremiseIndonesia TobaccoPas encore d'évaluation
- SingaporeDocument1 pageSingaporeIndonesia TobaccoPas encore d'évaluation
- ThailandDocument1 pageThailandIndonesia TobaccoPas encore d'évaluation
- MalaysiaDocument1 pageMalaysiaIndonesia TobaccoPas encore d'évaluation
- MauritusDocument1 pageMauritusIndonesia TobaccoPas encore d'évaluation
- IranDocument1 pageIranIndonesia TobaccoPas encore d'évaluation
- LatviaDocument1 pageLatviaIndonesia TobaccoPas encore d'évaluation
- CanadaDocument2 pagesCanadaIndonesia TobaccoPas encore d'évaluation
- IndiaDocument1 pageIndiaIndonesia TobaccoPas encore d'évaluation
- JordanDocument1 pageJordanIndonesia TobaccoPas encore d'évaluation
- EgyptDocument1 pageEgyptIndonesia TobaccoPas encore d'évaluation
- Googling Collection-The Web Authors Collected The Pictures Through Google. All Pictures Belong To Their Respective OwnersDocument16 pagesGoogling Collection-The Web Authors Collected The Pictures Through Google. All Pictures Belong To Their Respective OwnersIndonesia TobaccoPas encore d'évaluation
- DunhillDocument1 pageDunhillIndonesia TobaccoPas encore d'évaluation
- BrazilDocument2 pagesBrazilIndonesia TobaccoPas encore d'évaluation
- BruneiDocument1 pageBruneiIndonesia TobaccoPas encore d'évaluation
- AustraliaDocument4 pagesAustraliaIndonesia TobaccoPas encore d'évaluation
- VenezuelaDocument2 pagesVenezuelaIndonesia TobaccoPas encore d'évaluation
- DjarumDocument4 pagesDjarumIndonesia TobaccoPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Gamechanger by Bien Eli NillosDocument2 pagesThe Gamechanger by Bien Eli NillosBien Elli NillosPas encore d'évaluation
- Dario Diabetes Management App User ManualDocument12 pagesDario Diabetes Management App User ManualUdhaw KumarPas encore d'évaluation
- Cover Letter For Lab Research AssistantDocument6 pagesCover Letter For Lab Research Assistantf5b2q8e3100% (2)
- Uas Pak Alih Tugas KelompokDocument12 pagesUas Pak Alih Tugas KelompokMurni MebelPas encore d'évaluation
- Leadership in Healthcare Essential Values and Skills Third Edition PDF Version PDFDocument42 pagesLeadership in Healthcare Essential Values and Skills Third Edition PDF Version PDFmarilyn.llamas494100% (38)
- Germiston +27833736090 Dr. Jabulile/cheap Abortion Pills 4 Sale in Germiston/johannesburg ClinicDocument1 pageGermiston +27833736090 Dr. Jabulile/cheap Abortion Pills 4 Sale in Germiston/johannesburg Clinicsseruwagi miyodiPas encore d'évaluation
- Sexual and Reproductive Health and RightsDocument21 pagesSexual and Reproductive Health and RightsEmmanuelPas encore d'évaluation
- Duties and Responsibilities of A Midwife in RhuDocument6 pagesDuties and Responsibilities of A Midwife in RhuAlma PotentePas encore d'évaluation
- Muhimbili University of Health and Allied Sciences (Muhas) : For The Academic Year 2020/2021Document4 pagesMuhimbili University of Health and Allied Sciences (Muhas) : For The Academic Year 2020/2021Alfred JacksonPas encore d'évaluation
- Hand Reflexology-Key To Perfect HealthDocument340 pagesHand Reflexology-Key To Perfect Healthpadoita01100% (1)
- Physiotherapy Management For Patient With Primary Spontaneous Pneumothorax Dextra: A Case StudyDocument5 pagesPhysiotherapy Management For Patient With Primary Spontaneous Pneumothorax Dextra: A Case Studyjavier garzonPas encore d'évaluation
- GSA - Hatchery Standard - Issue 2.1 - 30-January-2023Document75 pagesGSA - Hatchery Standard - Issue 2.1 - 30-January-2023faribaPas encore d'évaluation
- Mirabel Halikhik 03Document1 pageMirabel Halikhik 03Dexter FumarPas encore d'évaluation
- Nigerian HeritageDocument156 pagesNigerian HeritageBarakat Adegboyega0% (1)
- EVS REPORT-coronaDocument38 pagesEVS REPORT-coronasekarchand33Pas encore d'évaluation
- Induction of Parturition and Termination of PregnancyDocument30 pagesInduction of Parturition and Termination of PregnancyVet IrfanPas encore d'évaluation
- BON 410 (Tutorial 1 & 2 With Solutions, 2023)Document11 pagesBON 410 (Tutorial 1 & 2 With Solutions, 2023)GrethePas encore d'évaluation
- Psychotropic DrugsDocument2 pagesPsychotropic DrugsMj BrionesPas encore d'évaluation
- About Palliative Care in India: Karunashraya - A Case StudyDocument4 pagesAbout Palliative Care in India: Karunashraya - A Case StudySayak ChakrabortyPas encore d'évaluation
- Letter - For - Students - 1ST - Year - Programmes (Gu)Document2 pagesLetter - For - Students - 1ST - Year - Programmes (Gu)Ayush SinghPas encore d'évaluation
- Turning Mindfulness Into AvoidanceDocument7 pagesTurning Mindfulness Into AvoidanceQuique ParadaPas encore d'évaluation
- Peace Corps Violation of Office of Victim Advocate Clearances by OVA Employee DI-16-0254 WB CommentsDocument26 pagesPeace Corps Violation of Office of Victim Advocate Clearances by OVA Employee DI-16-0254 WB CommentsAccessible Journal Media: Peace Corps DocumentsPas encore d'évaluation
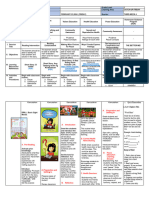
- DLL Catch Up Friday Week 4Document16 pagesDLL Catch Up Friday Week 4Maryanne Labaso93% (27)
- Drug Addiction RehabDocument10 pagesDrug Addiction RehabLorraine CashPas encore d'évaluation
- Adime 2Document10 pagesAdime 2api-307103979Pas encore d'évaluation
- ch02 (Lecture) - Workforce Safety and WellnessDocument63 pagesch02 (Lecture) - Workforce Safety and WellnessJomar TeofiloPas encore d'évaluation
- Reliability in Medical Device IndustryDocument14 pagesReliability in Medical Device IndustrySubramani KarurPas encore d'évaluation
- Gastrointestinal System Review QuestionsDocument10 pagesGastrointestinal System Review QuestionsSiena PlacinoPas encore d'évaluation
- Week 4 Ortho TestsDocument15 pagesWeek 4 Ortho Testsapi-468597987Pas encore d'évaluation
- Anti-Lock Braking System (ABS) For Trucks ... - Meritor WABCO PDFDocument112 pagesAnti-Lock Braking System (ABS) For Trucks ... - Meritor WABCO PDFEudis PinedaPas encore d'évaluation