Vous aimerez peut-être aussi
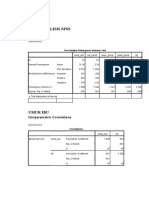
- SPSS ANALYSIS RESULTSDocument3 pagesSPSS ANALYSIS RESULTSPracinthya Dwitya PutriPas encore d'évaluation
- Peran Serta Suami Terhadap Ibu HamilDocument17 pagesPeran Serta Suami Terhadap Ibu HamilThallita Rahma Ziharviardy0% (1)
- Pemeriksaan ThoraxDocument27 pagesPemeriksaan ThoraxYaasinta ArlaesPas encore d'évaluation
- Presentation and Management of Nasopharyngeal Carcinoma, A Rare ChildhoodDocument3 pagesPresentation and Management of Nasopharyngeal Carcinoma, A Rare ChildhoodPracinthya Dwitya PutriPas encore d'évaluation
- Oo Aj 16000145Document4 pagesOo Aj 16000145Pracinthya Dwitya PutriPas encore d'évaluation
- Oo Aj 16000145Document4 pagesOo Aj 16000145Pracinthya Dwitya PutriPas encore d'évaluation
- 67 1455188856Document4 pages67 1455188856Pracinthya Dwitya PutriPas encore d'évaluation
- Anemia During PregnancyDocument8 pagesAnemia During Pregnancyekaseptiani312Pas encore d'évaluation
- Anemia During PregnancyDocument8 pagesAnemia During Pregnancyekaseptiani312Pas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Psychological Aspects of "A Beautiful Mind"Document12 pagesThe Psychological Aspects of "A Beautiful Mind"Azba Butt0% (1)
- Introduction to Insurance Agents and Customer ServiceDocument46 pagesIntroduction to Insurance Agents and Customer ServicePolireddy Venna100% (2)
- CH 9-10 Ethical Demensions 6thDocument70 pagesCH 9-10 Ethical Demensions 6thSteven ChikPas encore d'évaluation
- Chapter 5 - The Posterior Pituitary (Neurohypophysis)Document23 pagesChapter 5 - The Posterior Pituitary (Neurohypophysis)張宏軒Pas encore d'évaluation
- Minister of Health South Africa Update On CoronavirusDocument2 pagesMinister of Health South Africa Update On CoronavirusVučko IgorPas encore d'évaluation
- Microbiology IntroductionDocument2 pagesMicrobiology IntroductionAnonymous XuiUo2ThPas encore d'évaluation
- Case Presentation OB - GYNDocument14 pagesCase Presentation OB - GYNRaidah Ayesha RazackPas encore d'évaluation
- Digital tools enhance clinical reasoningDocument7 pagesDigital tools enhance clinical reasoningCésar LeónPas encore d'évaluation
- 02AdvancedThinkAhead3 Term2 TL2Document4 pages02AdvancedThinkAhead3 Term2 TL2natachaPas encore d'évaluation
- TOC Prof Chintamanis Comprehensive Book On SurgeryDocument4 pagesTOC Prof Chintamanis Comprehensive Book On SurgeryKoustav ChakrabortyPas encore d'évaluation
- Herbal Medicine For EveryoneDocument63 pagesHerbal Medicine For EveryoneMaratus Solehah100% (2)
- Influenced by The Intake and Utilization of Nutrients: (Todhunter, 1970) .Document3 pagesInfluenced by The Intake and Utilization of Nutrients: (Todhunter, 1970) .Elvira GumiPas encore d'évaluation
- Deepbite & Open BiteDocument36 pagesDeepbite & Open BiteNoor Zia100% (1)
- BPPVDocument2 pagesBPPVGavin TexeirraPas encore d'évaluation
- WHO EHC 240 Eng PDFDocument752 pagesWHO EHC 240 Eng PDFopenid_mRbxHxDC100% (1)
- Circular Covid-19 Measures: INCO International Fz. Co. ح م ش ﺔﯾﻟودﻟا وﻛﻧاDocument2 pagesCircular Covid-19 Measures: INCO International Fz. Co. ح م ش ﺔﯾﻟودﻟا وﻛﻧاErin JohnsonPas encore d'évaluation
- Time For A Paradigm ShiftDocument6 pagesTime For A Paradigm ShiftDavid GarcíaPas encore d'évaluation
- Diabetes Mellitus e ComplicaçõesDocument12 pagesDiabetes Mellitus e ComplicaçõesDouglas OliveiraPas encore d'évaluation
- Health - Questions - Pdf-Igcse Biology WorksheetDocument22 pagesHealth - Questions - Pdf-Igcse Biology WorksheetPrincess KimPas encore d'évaluation
- Rash PotpourriDocument10 pagesRash PotpourriWillMonasHuertasPas encore d'évaluation
- Declaracion Conformidad IFMR-45-GeneFinder-COVID-19-Plus-RealAmp-KitDocument2 pagesDeclaracion Conformidad IFMR-45-GeneFinder-COVID-19-Plus-RealAmp-KitalexanderPas encore d'évaluation
- Treasures of VijayakarDocument116 pagesTreasures of Vijayakarsurya100% (1)
- Project in Mapeh (Health)Document8 pagesProject in Mapeh (Health)guache warrinPas encore d'évaluation
- Hartland Memorial Hospital Case StudyDocument26 pagesHartland Memorial Hospital Case StudyZubeen ShahPas encore d'évaluation
- Unani IntroductionDocument37 pagesUnani Introductionhabib_VPas encore d'évaluation
- Fucidin®: Product MonographDocument21 pagesFucidin®: Product MonographLeonita SabrinaPas encore d'évaluation
- BORLAND Douglas Infuluenza PDFDocument18 pagesBORLAND Douglas Infuluenza PDFJxson GomezPas encore d'évaluation
- Health Effects of Rancid OilsDocument3 pagesHealth Effects of Rancid OilsMaiden PEIPas encore d'évaluation
- Understanding Oligodendroglioma - The Rarest of All Brain CancersDocument2 pagesUnderstanding Oligodendroglioma - The Rarest of All Brain CancersChris RyanPas encore d'évaluation
- Diabetes Advances in Diagnosis and TreatmentDocument11 pagesDiabetes Advances in Diagnosis and TreatmentAbi GarciaPas encore d'évaluation