Vous aimerez peut-être aussi
- The Craving Mind From Cigarettes To Smartphones To Love - Why We Get Hooked and How We Can Break Bad Habits PDFDocument257 pagesThe Craving Mind From Cigarettes To Smartphones To Love - Why We Get Hooked and How We Can Break Bad Habits PDFJacques Savariau92% (13)
- Sample FNCPDocument10 pagesSample FNCProssbert21Pas encore d'évaluation
- Pelvic Organ ProlapseDocument68 pagesPelvic Organ ProlapseAlyanna CrisologoPas encore d'évaluation
- First Level of AssessmentDocument7 pagesFirst Level of AssessmentJai - Ho100% (1)
- Home Visit Plan2Document2 pagesHome Visit Plan2Bianca BasnilloPas encore d'évaluation
- FNCPDocument26 pagesFNCPSugar Capule - ManuelPas encore d'évaluation
- Initial Data Base CompleteDocument24 pagesInitial Data Base CompleteCarlo AniagPas encore d'évaluation
- Family Health Assessment FormDocument8 pagesFamily Health Assessment FormKevin Llorente50% (2)
- A Typology of Nursing Problems in Family Nursing PracticeDocument10 pagesA Typology of Nursing Problems in Family Nursing PracticeAnika Ajihil100% (2)
- FNCP, Rnking and Scaling, Home Visit PlanDocument6 pagesFNCP, Rnking and Scaling, Home Visit Planmarie100% (10)
- Injection Pump Test SpecificationsDocument3 pagesInjection Pump Test Specificationsadmin tigasaudaraPas encore d'évaluation
- Typology of Nursing Problems in Family Nursing PracticeDocument10 pagesTypology of Nursing Problems in Family Nursing PracticeElaiza Mae MedidasPas encore d'évaluation
- FNCPDocument3 pagesFNCPHera Pamela Buelis Batoy100% (1)
- Business Emails - Style and StructureDocument4 pagesBusiness Emails - Style and StructureFall Eljed100% (1)
- Prioritization FNCPDocument3 pagesPrioritization FNCPWyen CabatbatPas encore d'évaluation
- Initial Database FNCPDocument8 pagesInitial Database FNCPIris CabertePas encore d'évaluation
- Initial Data Base For Family Nursing PracticeDocument9 pagesInitial Data Base For Family Nursing PracticeAlyanna Crisologo100% (1)
- Citizen's Army Training (CAT) Is A Compulsory Military Training For High School Students. Fourth-Year High SchoolDocument2 pagesCitizen's Army Training (CAT) Is A Compulsory Military Training For High School Students. Fourth-Year High SchoolJgary Lagria100% (1)
- FCPDocument25 pagesFCPErl DrizPas encore d'évaluation
- FNCP RequirementsDocument10 pagesFNCP RequirementsKathrynne MendozaPas encore d'évaluation
- Initial Data Base For Family Nursing PracticeDocument13 pagesInitial Data Base For Family Nursing PracticeSj CapindingPas encore d'évaluation
- Movie ReviewDocument2 pagesMovie ReviewJohanna Gwenn Taganahan LomaadPas encore d'évaluation
- Related Learning Experience (RLE) Activity in NCM 104: Community Health Nursing 1 (Individual and Family) 1 Semester (A.Y. 2020-2021)Document5 pagesRelated Learning Experience (RLE) Activity in NCM 104: Community Health Nursing 1 (Individual and Family) 1 Semester (A.Y. 2020-2021)Borromeo, Kriztian Ralph O.Pas encore d'évaluation
- A. Family Structure, Characteristics and Dynamics TheDocument3 pagesA. Family Structure, Characteristics and Dynamics TheJessa_Krisma_T_1321100% (4)
- Family Health NursingDocument11 pagesFamily Health NursingKBD100% (1)
- Family Assessment Tool 2022 1Document3 pagesFamily Assessment Tool 2022 1stephanie serdoncilloPas encore d'évaluation
- Initial Data Base RleDocument17 pagesInitial Data Base Rlejeff_blur00388% (16)
- Shaping School Culture Case StudyDocument7 pagesShaping School Culture Case Studyapi-524477308Pas encore d'évaluation
- Family Case AnalysisDocument17 pagesFamily Case Analysisapi-3832358100% (9)
- FNCP - (1) SampleDocument8 pagesFNCP - (1) SampleLEONELLGABRIEL RAGUINDINPas encore d'évaluation
- FNCP SampleDocument36 pagesFNCP SampleLyka Milo AvilaPas encore d'évaluation
- Typology of Nursing Problems in Family Nursing PracticeDocument2 pagesTypology of Nursing Problems in Family Nursing PracticeHarlene Joyce Rey100% (3)
- Health DeficitDocument1 pageHealth DeficitJaime PorschePas encore d'évaluation
- Initial Data Base For Family Nursing PracticeDocument12 pagesInitial Data Base For Family Nursing Practicemiss RN67% (18)
- Family Coping IndexDocument3 pagesFamily Coping IndexJoanne PaestePas encore d'évaluation
- Febrile Seizure: Febrile Seizure, Also Known As A Fever Fit or Febrile Convulsion, IsDocument4 pagesFebrile Seizure: Febrile Seizure, Also Known As A Fever Fit or Febrile Convulsion, Isjdcrisologo8860Pas encore d'évaluation
- Family Care Plan of ROSARIO: (1 Level Assessment) (2 Level Assessment) (Specific)Document3 pagesFamily Care Plan of ROSARIO: (1 Level Assessment) (2 Level Assessment) (Specific)Eduard Reyjell MontañoPas encore d'évaluation
- Caterpillar Cat 304.5 Mini Hydraulic Excavator (Prefix WAK) Service Repair Manual (WAK00001 and Up)Document23 pagesCaterpillar Cat 304.5 Mini Hydraulic Excavator (Prefix WAK) Service Repair Manual (WAK00001 and Up)kfmuseddk100% (1)
- FNCP - DMDocument5 pagesFNCP - DMAndee SalegonPas encore d'évaluation
- FNCP Health CenterDocument3 pagesFNCP Health CenterEarl Ramos100% (4)
- Steps in Making A Family Nursing Care PlanDocument4 pagesSteps in Making A Family Nursing Care PlanMary LouPas encore d'évaluation
- Initial Data Base For Family Nursing PracticeDocument4 pagesInitial Data Base For Family Nursing PracticeCleoville OrdonaPas encore d'évaluation
- Propaganda TechniquesDocument4 pagesPropaganda TechniquesAlyanna CrisologoPas encore d'évaluation
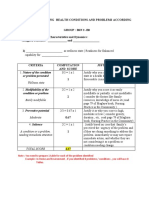
- Scale For Ranking Health Conditions and Problems According To Priorities-1Document3 pagesScale For Ranking Health Conditions and Problems According To Priorities-1Bee Anne BiñasPas encore d'évaluation
- Initial Data Base and FNCPDocument35 pagesInitial Data Base and FNCPRichard82% (11)
- Initial Data BaseDocument16 pagesInitial Data BaseJohn Philip M. Lacas RN0% (1)
- Initial Data Base For Family Nursing PracticeDocument13 pagesInitial Data Base For Family Nursing PracticeGamer Doge100% (1)
- Initial Data Base For Family Nursing PracticeDocument7 pagesInitial Data Base For Family Nursing PracticeMayls Sevilla Calizo0% (1)
- Initial Data Base For Family Nursing PracticeDocument18 pagesInitial Data Base For Family Nursing PracticeKenneth Mark B. TevesPas encore d'évaluation
- Initial Data Base For Family Nursing Practice: A. Family Structure Characteristics and DynamicsDocument3 pagesInitial Data Base For Family Nursing Practice: A. Family Structure Characteristics and DynamicsjajaPas encore d'évaluation
- Initial Database For Family Nursing PracticeDocument17 pagesInitial Database For Family Nursing PracticeLevi Cyr PerezPas encore d'évaluation
- Family Case Study: BLK 4. Room 7, Phase 5 Brgy. Dela PazDocument9 pagesFamily Case Study: BLK 4. Room 7, Phase 5 Brgy. Dela PazShamz SitiarPas encore d'évaluation
- Sample of IDBDocument3 pagesSample of IDBRJ Pots IbañezPas encore d'évaluation
- Initial Data Base For Family Nursing PracticeDocument8 pagesInitial Data Base For Family Nursing PracticeKiara Denise TamayoPas encore d'évaluation
- A Typology of Nursing Problems in Family Nursing PracticeDocument8 pagesA Typology of Nursing Problems in Family Nursing PracticeClifford Ogad0% (1)
- First Level AssessmentDocument2 pagesFirst Level AssessmentWenalyn Grace Abella LlavanPas encore d'évaluation
- FNCP PrioritizationDocument3 pagesFNCP PrioritizationKim Denice PunoPas encore d'évaluation
- CHN-RLE Module 2 (Home Visits)Document5 pagesCHN-RLE Module 2 (Home Visits)Ems Rio Bal100% (1)
- FNCP Category and PrioritizationDocument8 pagesFNCP Category and PrioritizationJapeth John M. FloresPas encore d'évaluation
- Editing.... - SCALE FOR RANKING HEALTH CONDITIONS AND PROBLEMS ACCORDING TO PRIORITIESDocument15 pagesEditing.... - SCALE FOR RANKING HEALTH CONDITIONS AND PROBLEMS ACCORDING TO PRIORITIESDonna Mae BoolPas encore d'évaluation
- FNCP Risk For InfectionDocument4 pagesFNCP Risk For InfectionAemz Alacasnap Ainegud0% (1)
- FSPR Masalunga1Document34 pagesFSPR Masalunga1Janela CaballesPas encore d'évaluation
- Family Health NursingDocument3 pagesFamily Health Nursingmarjo24100% (1)
- Initial Data Base For Family Nursing PracticeDocument15 pagesInitial Data Base For Family Nursing PracticeLyka SaysonPas encore d'évaluation
- Family Nursing PracticeDocument34 pagesFamily Nursing PracticeAisa Castro Arguelles100% (3)
- FNCP Prioritization SheetDocument3 pagesFNCP Prioritization SheetAndrea Franchesca DelaCruz DescalzoPas encore d'évaluation
- FNCP NewDocument29 pagesFNCP NewKhim Margarette DionisioPas encore d'évaluation
- CONDUCTING FAMILY HEALTH ASSESSMENT TOOL Geno Adrian T. Pampanga BSN-2ADocument11 pagesCONDUCTING FAMILY HEALTH ASSESSMENT TOOL Geno Adrian T. Pampanga BSN-2AGeno Adrian T PampangaPas encore d'évaluation
- Initial Data Base For Family Nursing PracticeDocument9 pagesInitial Data Base For Family Nursing PracticeMD PraxPas encore d'évaluation
- Family Health AssessmentDocument9 pagesFamily Health AssessmentCRYSTHAL S. DIBDIBPas encore d'évaluation
- Famacion - CHN Survey ToolDocument14 pagesFamacion - CHN Survey ToolKyra Bianca R. Famacion100% (1)
- Meal PlanDocument3 pagesMeal PlanAlyanna CrisologoPas encore d'évaluation
- OrganizingDocument6 pagesOrganizingAlyanna CrisologoPas encore d'évaluation
- Day 8 ScheduleDocument1 pageDay 8 ScheduleAlyanna CrisologoPas encore d'évaluation
- Day 8 ScheduleDocument1 pageDay 8 ScheduleAlyanna CrisologoPas encore d'évaluation
- School Health Care PlanDocument7 pagesSchool Health Care PlanAlyanna CrisologoPas encore d'évaluation
- Day 8 ScheduleDocument1 pageDay 8 ScheduleAlyanna CrisologoPas encore d'évaluation
- Respiratory FailureDocument6 pagesRespiratory FailureAlyanna CrisologoPas encore d'évaluation
- Counting Techniques AND ProbabilityDocument74 pagesCounting Techniques AND ProbabilityAlyanna Crisologo50% (2)
- Measures of Central TendencyDocument58 pagesMeasures of Central TendencyAlyanna CrisologoPas encore d'évaluation
- José Protacio Rizal Mercado y Alonso RealondaDocument8 pagesJosé Protacio Rizal Mercado y Alonso RealondaAlyanna CrisologoPas encore d'évaluation
- Chapter 1Document41 pagesChapter 1Alyanna CrisologoPas encore d'évaluation
- Clonidine HydrochlorideDocument3 pagesClonidine HydrochlorideAlyanna CrisologoPas encore d'évaluation
- Acute GastroenteritisDocument2 pagesAcute GastroenteritisAlyanna CrisologoPas encore d'évaluation
- A Mating RelationshipDocument7 pagesA Mating RelationshipAlyanna CrisologoPas encore d'évaluation
- Students JournalDocument12 pagesStudents JournalAlyanna CrisologoPas encore d'évaluation
- Asthma: Common Asthma Triggers Include: Signs and SymptomsDocument3 pagesAsthma: Common Asthma Triggers Include: Signs and SymptomsAlyanna CrisologoPas encore d'évaluation
- Simple Machines TestDocument7 pagesSimple Machines TestAlyanna CrisologoPas encore d'évaluation
- ParentGuide EnglishDocument28 pagesParentGuide EnglishAlyanna CrisologoPas encore d'évaluation
- Opinion2008 190Document2 pagesOpinion2008 190Alyanna CrisologoPas encore d'évaluation
- (G.R. NO. 173253, October 30, 2006) : Garcia, J.Document19 pages(G.R. NO. 173253, October 30, 2006) : Garcia, J.Alyanna CrisologoPas encore d'évaluation
- Parent Guide EnglishDocument28 pagesParent Guide EnglishVK RAJENDRANPas encore d'évaluation
- House Okays Bill Extending Period To Rectify Simulated BirthsDocument1 pageHouse Okays Bill Extending Period To Rectify Simulated BirthsAlyanna CrisologoPas encore d'évaluation
- Do or Does1.1.2Document4 pagesDo or Does1.1.2dzanardipintoPas encore d'évaluation
- LEARNING MODULE Entrep Lesson 1-2Document19 pagesLEARNING MODULE Entrep Lesson 1-2Cindy BononoPas encore d'évaluation
- Upload A Document To Access Your Download: Social Studies of HealthDocument3 pagesUpload A Document To Access Your Download: Social Studies of Health1filicupEPas encore d'évaluation
- Houses WorksheetDocument3 pagesHouses WorksheetYeferzon Clavijo GilPas encore d'évaluation
- Project Management Pro: Powerpoint SlidesDocument350 pagesProject Management Pro: Powerpoint SlidesJosephPas encore d'évaluation
- BeneHeart D3 Defibrillator Product BrochureDocument4 pagesBeneHeart D3 Defibrillator Product BrochureJasmine Duan100% (1)
- VVP Engg. CollegeDocument32 pagesVVP Engg. Collegechotaimanav17Pas encore d'évaluation
- The SU Electric Fuel Pump Type Car Reference List AUA 214Document4 pagesThe SU Electric Fuel Pump Type Car Reference List AUA 214Anonymous aOXD9JuqdPas encore d'évaluation
- Phil. Organic ActDocument15 pagesPhil. Organic Actka travelPas encore d'évaluation
- Orca Share Media1579045614947Document4 pagesOrca Share Media1579045614947Teresa Marie Yap CorderoPas encore d'évaluation
- Model United Nations at Home Code of ConductDocument3 pagesModel United Nations at Home Code of ConductAryan KashyapPas encore d'évaluation
- Abb PB - Power-En - e PDFDocument16 pagesAbb PB - Power-En - e PDFsontungPas encore d'évaluation
- LMR - 2023 04 14Document5 pagesLMR - 2023 04 14Fernando ShitinoePas encore d'évaluation
- Labor Law Highlights, 1915-2015: Labor Review Has Been in Publication. All The LegislationDocument13 pagesLabor Law Highlights, 1915-2015: Labor Review Has Been in Publication. All The LegislationIgu jumaPas encore d'évaluation
- Decemeber 2020 Examinations: Suggested Answers ToDocument41 pagesDecemeber 2020 Examinations: Suggested Answers ToDipen AdhikariPas encore d'évaluation
- The Organization of PericentroDocument33 pagesThe Organization of PericentroTunggul AmetungPas encore d'évaluation
- 14 BibiliographyDocument22 pages14 BibiliographyvaibhavPas encore d'évaluation
- 2 - (Accounting For Foreign Currency Transaction)Document25 pages2 - (Accounting For Foreign Currency Transaction)Stephiel SumpPas encore d'évaluation
- Leadership and Turnaround Management Concepts Applied in The Agribusiness Environment in RomaniaDocument6 pagesLeadership and Turnaround Management Concepts Applied in The Agribusiness Environment in RomaniaLoredana PredaPas encore d'évaluation
- Case Study - Lucky Cement and OthersDocument16 pagesCase Study - Lucky Cement and OthersKabeer QureshiPas encore d'évaluation
- TestertDocument10 pagesTestertjaiPas encore d'évaluation
- SMTP/POP3/IMAP Email Engine Library For C/C++ Programmer's ManualDocument40 pagesSMTP/POP3/IMAP Email Engine Library For C/C++ Programmer's Manualadem ademPas encore d'évaluation
- Multigrade Lesson Plan MathDocument7 pagesMultigrade Lesson Plan MathArmie Yanga HernandezPas encore d'évaluation