Vous aimerez peut-être aussi
- Rifaximin Nihms443516Document10 pagesRifaximin Nihms443516MIHAELAPas encore d'évaluation
- TB Case StudyDocument2 pagesTB Case StudyReisabelle LabianoPas encore d'évaluation
- PGI MANIMTIM - COVID-19 in PregnancyDocument1 pagePGI MANIMTIM - COVID-19 in PregnancyKim Adarem Joy ManimtimPas encore d'évaluation
- Aspiration PneumoniaDocument3 pagesAspiration PneumoniaEllen Hennings100% (1)
- Zocor (Simvastatin)Document3 pagesZocor (Simvastatin)E100% (1)
- Hyperthermia: A Nursing Care Plan Presented To Maria Catherine Belarma, RN, MNDocument6 pagesHyperthermia: A Nursing Care Plan Presented To Maria Catherine Belarma, RN, MNJanelle NarcisoPas encore d'évaluation
- TOF (Pathophysiology)Document4 pagesTOF (Pathophysiology)Doreen Claire M. WallangPas encore d'évaluation
- Kardex, Drug Study and CheckDocument12 pagesKardex, Drug Study and CheckJemina Rafanan RacadioPas encore d'évaluation
- Importance of Honesty in MedicineDocument3 pagesImportance of Honesty in MedicineSuiweng WongPas encore d'évaluation
- A Case Study On Graves DiseaseDocument46 pagesA Case Study On Graves DiseaseRenie SerranoPas encore d'évaluation
- What Is Prednisolone?Document12 pagesWhat Is Prednisolone?Chandni SeelochanPas encore d'évaluation
- USC Case 04 - SinusitisDocument9 pagesUSC Case 04 - SinusitisDisti Damelia SebayangPas encore d'évaluation
- BSN4D-SG2 DM Type2Document201 pagesBSN4D-SG2 DM Type2Charisse CaydanPas encore d'évaluation
- Pathophysiology of Covid-19 Infection: What Is The Novel Coronavirus (Sars-Cov-2) Doing To Body? A Comprehensive Systematic ReviewDocument15 pagesPathophysiology of Covid-19 Infection: What Is The Novel Coronavirus (Sars-Cov-2) Doing To Body? A Comprehensive Systematic ReviewMade DeanaPas encore d'évaluation
- Atropine: Drug Study: NCM 106 PharmacologyDocument6 pagesAtropine: Drug Study: NCM 106 PharmacologyKevin RosalesPas encore d'évaluation
- Case Study PcapDocument3 pagesCase Study PcapClaire PalaciosPas encore d'évaluation
- Drug Study Copd FinalDocument3 pagesDrug Study Copd FinalMaverick LimPas encore d'évaluation
- Quiz LeukemiaDocument4 pagesQuiz LeukemiaHanna La MadridPas encore d'évaluation
- Pneumonia Case Study FinalllDocument56 pagesPneumonia Case Study Finalllbethrice melegritoPas encore d'évaluation
- Pediatric Community Acquired Pneumonia - Moderate Risk: University of The Cordilleras College of NursingDocument22 pagesPediatric Community Acquired Pneumonia - Moderate Risk: University of The Cordilleras College of NursingJemimah AdaclogPas encore d'évaluation
- Pediatrics Community Acquired PneumoniaDocument2 pagesPediatrics Community Acquired PneumoniaLizaMariePas encore d'évaluation
- Case Study PneumoniaDocument14 pagesCase Study PneumoniaJester GalayPas encore d'évaluation
- Tetralogy of FallotDocument3 pagesTetralogy of FallotJohn Mark PocsidioPas encore d'évaluation
- Pediatric Community Acquired PneumoniaDocument24 pagesPediatric Community Acquired PneumoniaJames Lagamayo JavierPas encore d'évaluation
- Case Study 1 (Pneumonia)Document13 pagesCase Study 1 (Pneumonia)Kate EscotonPas encore d'évaluation
- PTB Case-StudyDocument64 pagesPTB Case-StudyBeverly DatuPas encore d'évaluation
- Drug Study Paracetamol Ambroxol Ascorbic Acid CefuroximeDocument6 pagesDrug Study Paracetamol Ambroxol Ascorbic Acid CefuroximeJaymark LambinoPas encore d'évaluation
- Acute Bronchitis Care Study 202Document25 pagesAcute Bronchitis Care Study 202Kara Kathrina Fuentes100% (1)
- NCM 112 Rle Care of Client With Alteration in Oxygenation: A Case Study On: Chronic Obstructive Pulmonary DiseaseDocument24 pagesNCM 112 Rle Care of Client With Alteration in Oxygenation: A Case Study On: Chronic Obstructive Pulmonary DiseaseMadelyn SerneoPas encore d'évaluation
- Pathognomonic Signs of Communicable Diseases: JJ8009 Health & NutritionDocument2 pagesPathognomonic Signs of Communicable Diseases: JJ8009 Health & NutritionMauliza Resky NisaPas encore d'évaluation
- NCP IcuDocument2 pagesNCP IcuDiana MuañaPas encore d'évaluation
- MedSurg Notes - Cancer of The LiverDocument2 pagesMedSurg Notes - Cancer of The LiverMae CeaesarPas encore d'évaluation
- PneumoniaDocument1 pagePneumoniaAyen FornollesPas encore d'évaluation
- Care Study Pneumonia SampleDocument28 pagesCare Study Pneumonia SampleKaloy KamaoPas encore d'évaluation
- Drug StudyDocument7 pagesDrug StudyGladys NacionPas encore d'évaluation
- Preeclampsia Pathophysiology and ManagementDocument7 pagesPreeclampsia Pathophysiology and ManagementAuliaPas encore d'évaluation
- Aspiration PneumoniaDocument27 pagesAspiration PneumoniaReya Awali SuasoPas encore d'évaluation
- Ward Case PresentationDocument92 pagesWard Case PresentationSuzette Rae TatePas encore d'évaluation
- 4 .unit-IVDocument73 pages4 .unit-IVPriya bhattiPas encore d'évaluation
- Case Study PTBDocument3 pagesCase Study PTBApril Imperial Tordecillas100% (1)
- Schematic Diagram BA HAP HRDocument2 pagesSchematic Diagram BA HAP HRMika MinsalanPas encore d'évaluation
- Bacillary DysenteryDocument32 pagesBacillary Dysenteryapi-199163990% (1)
- PCAPDocument2 pagesPCAPMizpah DuculanPas encore d'évaluation
- I.intrODUCTION Hypertension (High Blood Pressure) Is ADocument19 pagesI.intrODUCTION Hypertension (High Blood Pressure) Is Aoril04Pas encore d'évaluation
- D. Pa Tho Physiology of PneumoniaDocument4 pagesD. Pa Tho Physiology of PneumoniaBill Clinton Lamira BabanPas encore d'évaluation
- Hyaline Membrane DiseaseDocument31 pagesHyaline Membrane DiseaseWeng RamojalPas encore d'évaluation
- Community-Acquired Pneumonia: Bello, Mickaela Bianca A. Gumiran, NomerDocument37 pagesCommunity-Acquired Pneumonia: Bello, Mickaela Bianca A. Gumiran, NomerKristine-Joy Legaspi FrancoPas encore d'évaluation
- Pneumonia Teaching PlanDocument5 pagesPneumonia Teaching PlanRaghav RoyPas encore d'évaluation
- BPNDocument49 pagesBPNlovelots1234100% (1)
- Drug Study: Name Mechanism of Action Indication/Contraindication Side Effects Nursing ResponsibilityDocument2 pagesDrug Study: Name Mechanism of Action Indication/Contraindication Side Effects Nursing ResponsibilityJoshua DavantesPas encore d'évaluation
- Nursing Theory: Asthma (Presentation)Document13 pagesNursing Theory: Asthma (Presentation)vinda astri permatasari100% (1)
- Occurs Most Often In:: Muscular DystrophyDocument4 pagesOccurs Most Often In:: Muscular DystrophyJiezl Abellano AfinidadPas encore d'évaluation
- ProcreationDocument55 pagesProcreationRoshin TejeroPas encore d'évaluation
- Case 5 SeizureDocument74 pagesCase 5 SeizureGrace TanajuraPas encore d'évaluation
- Hematologic Disorders Test Drill For Ikonek 2Document4 pagesHematologic Disorders Test Drill For Ikonek 2Jan Cyrel ColomaPas encore d'évaluation
- Community Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsD'EverandCommunity Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsPas encore d'évaluation
- The LungsDocument5 pagesThe LungsMacmac CAsPas encore d'évaluation
- 1-The Respiratory SystemDocument7 pages1-The Respiratory SystemEma FröhlichováPas encore d'évaluation
- Anatomi Fisiologi Sistem Pernafasan - Id.enDocument7 pagesAnatomi Fisiologi Sistem Pernafasan - Id.enCindy Ari SantiPas encore d'évaluation
- ThesisDocument58 pagesThesisTirtha Roy BiswasPas encore d'évaluation
- Friedman LawsuitDocument12 pagesFriedman LawsuitChris GothnerPas encore d'évaluation
- Corporation Law Case Digests Philippines Merger and ConsolidationDocument7 pagesCorporation Law Case Digests Philippines Merger and ConsolidationAlpha BetaPas encore d'évaluation
- Quarter 2-Module 7 Social and Political Stratification: Department of Education Republic of The PhilippinesDocument21 pagesQuarter 2-Module 7 Social and Political Stratification: Department of Education Republic of The Philippinestricia100% (5)
- Role of Courts in Granting Bails and Bail Reforms: TH THDocument1 pageRole of Courts in Granting Bails and Bail Reforms: TH THSamarth VikramPas encore d'évaluation
- ThermodynamicsDocument341 pagesThermodynamicsjonathan2788100% (4)
- Chemiphase Oilfield Demulsifier Testing ProcedureDocument4 pagesChemiphase Oilfield Demulsifier Testing ProcedureBen Wiggins100% (1)
- E 18 - 02 - Rte4ltay PDFDocument16 pagesE 18 - 02 - Rte4ltay PDFvinoth kumar SanthanamPas encore d'évaluation
- Man Is Made by His BeliefDocument2 pagesMan Is Made by His BeliefLisa KireechevaPas encore d'évaluation
- Acidity (As Acetic Acid) On Undenatured and Denatured EthanolDocument10 pagesAcidity (As Acetic Acid) On Undenatured and Denatured EthanolVinh NguyenPas encore d'évaluation
- Brochure 8 VT 8Document24 pagesBrochure 8 VT 8David GonzalesPas encore d'évaluation
- Case - Marico SCMDocument26 pagesCase - Marico SCMChandan Gupta50% (2)
- Adolescent Violence Towards Parents Myths and RealitiesDocument25 pagesAdolescent Violence Towards Parents Myths and RealitiesJoão D C MendonçaPas encore d'évaluation
- 9.2 Volumetric Analysis PDFDocument24 pages9.2 Volumetric Analysis PDFJoaquinPas encore d'évaluation
- Interfaces and Inheritance in JavaDocument1 pageInterfaces and Inheritance in JavaegdejuanaPas encore d'évaluation
- J of Cosmetic Dermatology - 2019 - Zhang - A Cream of Herbal Mixture To Improve MelasmaDocument8 pagesJ of Cosmetic Dermatology - 2019 - Zhang - A Cream of Herbal Mixture To Improve Melasmaemily emiPas encore d'évaluation
- Canon Law Eng. Appunti Part 2Document91 pagesCanon Law Eng. Appunti Part 2noelPas encore d'évaluation
- Public BudgetingDocument15 pagesPublic BudgetingTom Wan Der100% (4)
- Welcome To The Jfrog Artifactory User Guide!Document3 pagesWelcome To The Jfrog Artifactory User Guide!RaviPas encore d'évaluation
- Memory and History in The Folklores Reinvented Through BeowulfDocument10 pagesMemory and History in The Folklores Reinvented Through BeowulfDebojyoti DanPas encore d'évaluation
- Reaction PaperDocument3 pagesReaction PaperCecille Robles San JosePas encore d'évaluation
- CHAPTER 4 (B)Document6 pagesCHAPTER 4 (B)Jon Lester De VeyraPas encore d'évaluation
- Class 12 Accountancy HHDocument58 pagesClass 12 Accountancy HHkomal barotPas encore d'évaluation
- Different Departments Required in A HospitalDocument11 pagesDifferent Departments Required in A HospitalEdsel Dudes AbantePas encore d'évaluation
- Analysing Worship in The Pentateuch and Its ApplicationDocument12 pagesAnalysing Worship in The Pentateuch and Its ApplicationDaniel Solomon100% (1)
- LakmeDocument34 pagesLakmeSuraj Pratap Sawhney79% (14)
- Storey Publishing Fall 2017 CatalogDocument108 pagesStorey Publishing Fall 2017 CatalogStorey PublishingPas encore d'évaluation
- Asset Management PlanDocument160 pagesAsset Management Planbkalatus1100% (1)
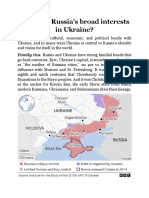
- What Are RussiaDocument3 pagesWhat Are RussiaMuhammad SufyanPas encore d'évaluation
- Final Research ReportDocument14 pagesFinal Research ReportAlojado Lamuel Jesu APas encore d'évaluation