Vous aimerez peut-être aussi
- Autonomic Nervous System & Homeopathy: Personalized Nutrition Concept Depicted in Homeopathy & AyurvedaD'EverandAutonomic Nervous System & Homeopathy: Personalized Nutrition Concept Depicted in Homeopathy & AyurvedaPas encore d'évaluation
- A Review On Antidepressant Plants: Available Online ThroughDocument15 pagesA Review On Antidepressant Plants: Available Online ThroughIra AiniPas encore d'évaluation
- Articulo Adaptogenicos Estres PDFDocument6 pagesArticulo Adaptogenicos Estres PDFJaime CuelloPas encore d'évaluation
- Chinese Phytotherapy To Reduce Stress, Anxiety and Improve Quality of Life: Randomized Controlled TrialDocument8 pagesChinese Phytotherapy To Reduce Stress, Anxiety and Improve Quality of Life: Randomized Controlled Trialthunder.egePas encore d'évaluation
- Herbal Sources of Antidepressant Potential A Review PDFDocument6 pagesHerbal Sources of Antidepressant Potential A Review PDFNestor D. Mores, Jr.Pas encore d'évaluation
- Medicine: The Effectiveness of Tai Chi For Postpartum DepressionDocument4 pagesMedicine: The Effectiveness of Tai Chi For Postpartum DepressionNisa RohmatinPas encore d'évaluation
- ST John's Wort - YDGLDocument13 pagesST John's Wort - YDGLDessirhe LaraPas encore d'évaluation
- Journal of Herbal PlantsDocument8 pagesJournal of Herbal PlantsDesy MeldawatiPas encore d'évaluation
- Curcumin For Depression: A Meta-Analysis: Critical Reviews in Food Science and NutritionDocument12 pagesCurcumin For Depression: A Meta-Analysis: Critical Reviews in Food Science and NutritionCrish Tatiana C. SuaznabarPas encore d'évaluation
- Folic Acid Ameliorates Depression-Like - JÁ FOIDocument8 pagesFolic Acid Ameliorates Depression-Like - JÁ FOICamila VasquesPas encore d'évaluation
- Pharmacophore: Nazanin Farrokhi, Fatemeh Yousefzadeh, Mir Majid Saeedi, Leila Behnam, Shahrbanoo GhahariDocument8 pagesPharmacophore: Nazanin Farrokhi, Fatemeh Yousefzadeh, Mir Majid Saeedi, Leila Behnam, Shahrbanoo GhahariDestri DhelianaPas encore d'évaluation
- Physical Exercise and Major Depressive Disorder in Adults Systematic Review and Meta AnalysisDocument17 pagesPhysical Exercise and Major Depressive Disorder in Adults Systematic Review and Meta AnalysisErick NunesPas encore d'évaluation
- Classical Psychedelics For The Treatment of Depression and AnxietyDocument14 pagesClassical Psychedelics For The Treatment of Depression and AnxietyAnonymous FjTisojPas encore d'évaluation
- Journal of Ginseng Research: Seungyeop Lee, Dong-Kwon RheeDocument6 pagesJournal of Ginseng Research: Seungyeop Lee, Dong-Kwon Rheenermal93Pas encore d'évaluation
- tdgx00Document10 pagestdgx00Leonardo De Moro FerreiraPas encore d'évaluation
- The Use of Medicinal Plants in The Treatment of Mental Disorders: An OverviewDocument5 pagesThe Use of Medicinal Plants in The Treatment of Mental Disorders: An Overviewvenkat rajuPas encore d'évaluation
- Major Depressive Disorder Pathophysiology and Clinical Management 2167 1044 1000255Document8 pagesMajor Depressive Disorder Pathophysiology and Clinical Management 2167 1044 1000255Wanda HamidahPas encore d'évaluation
- 1 s2.0 S2213422019300150 MainDocument6 pages1 s2.0 S2213422019300150 MainMonaPas encore d'évaluation
- CNS Plant Therapy For Post-Traumatic Stress DisorderDocument14 pagesCNS Plant Therapy For Post-Traumatic Stress DisorderInternational Journal of Innovative Science and Research TechnologyPas encore d'évaluation
- Depression in Patients With Multiple Sclerosis: A Review StudyDocument5 pagesDepression in Patients With Multiple Sclerosis: A Review StudyalirezanouriPas encore d'évaluation
- Treatment Options For Insomnia: Kalyanakrishnan Ramakrishnan, MD, and Dewey C. Scheid, MD, MPHDocument10 pagesTreatment Options For Insomnia: Kalyanakrishnan Ramakrishnan, MD, and Dewey C. Scheid, MD, MPHJhonny BatongPas encore d'évaluation
- HHS Public Access: Fish Oil and Depression: The Skinny On FatsDocument13 pagesHHS Public Access: Fish Oil and Depression: The Skinny On FatsIqbal AbdillahPas encore d'évaluation
- Nada Ear Acupressure For Covid19 Stress ManagementDocument7 pagesNada Ear Acupressure For Covid19 Stress ManagementCamille EgidioPas encore d'évaluation
- Depression - A Narrative SynthesisDocument15 pagesDepression - A Narrative SynthesisShiv Thakare FanPas encore d'évaluation
- The Association of Dietary Inflammatory Potential With Depre - 2017 - PreventiveDocument7 pagesThe Association of Dietary Inflammatory Potential With Depre - 2017 - Preventivegiulia.santinPas encore d'évaluation
- Comparing Mindfulness Based Cognitive THDocument5 pagesComparing Mindfulness Based Cognitive THolgasacristan316Pas encore d'évaluation
- Effectiveness of Group Reminiscence Therapy On Depression Among The Institutionalized ElderlyDocument8 pagesEffectiveness of Group Reminiscence Therapy On Depression Among The Institutionalized ElderlyIJAR JOURNALPas encore d'évaluation
- The Role of Psychotropic Medications in The ManagementDocument24 pagesThe Role of Psychotropic Medications in The ManagementloloasbPas encore d'évaluation
- Chinese Herbal Formula Xiao Yao San ForDocument14 pagesChinese Herbal Formula Xiao Yao San ForJamila IthaiaPas encore d'évaluation
- Trastorno Depresivo en Edades TempranasDocument15 pagesTrastorno Depresivo en Edades TempranasManuel Dacio Castañeda CabelloPas encore d'évaluation
- Bekam Migren PDFDocument27 pagesBekam Migren PDFJuan Scoter'sPas encore d'évaluation
- 2.2psylocibin-Assisted Therapy For Depression - Craig PearsonDocument9 pages2.2psylocibin-Assisted Therapy For Depression - Craig PearsonMarcos Vinicius Cieri de MouraPas encore d'évaluation
- Morbid Anxiety As A Risk Factor in Patients With Somatic Diseases A Review of Recent FindingsDocument9 pagesMorbid Anxiety As A Risk Factor in Patients With Somatic Diseases A Review of Recent FindingsAdelina AndritoiPas encore d'évaluation
- And Challenges: Physical Activity As A Clinical Tool Against Depression: OpportunitiesDocument14 pagesAnd Challenges: Physical Activity As A Clinical Tool Against Depression: OpportunitiesfitrianiPas encore d'évaluation
- Ayurvedic Medicinal Plants For Alzheimer's DiseaseDocument9 pagesAyurvedic Medicinal Plants For Alzheimer's Diseasejcamacho95Pas encore d'évaluation
- The Efficacy of Hope Therapy On The Elderly Depression in Mehriz Day Care CentersDocument6 pagesThe Efficacy of Hope Therapy On The Elderly Depression in Mehriz Day Care CentersDevy Oktavia AnisaPas encore d'évaluation
- Therapeutic Effects of Phytochemicals and MedicinaDocument11 pagesTherapeutic Effects of Phytochemicals and MedicinaMd. JubairPas encore d'évaluation
- Panss ScoreDocument8 pagesPanss ScoretriaclaresiaPas encore d'évaluation
- Fluoxetine Versus Nortryptiline in Treatment of DepressionDocument7 pagesFluoxetine Versus Nortryptiline in Treatment of DepressionwybcxkPas encore d'évaluation
- Mind Body IntervensiDocument5 pagesMind Body IntervensiSyarief NursePas encore d'évaluation
- Various Authors - Brain Activity in Sleep Compared To WakefulnessDocument24 pagesVarious Authors - Brain Activity in Sleep Compared To WakefulnessDestriPas encore d'évaluation
- Journal of Ayurveda and Integrative MedicineDocument4 pagesJournal of Ayurveda and Integrative MedicineMiftakhul ViviPas encore d'évaluation
- Efectos de La Manipulacion Esteopatica en El Desrden General de AnsiedadDocument11 pagesEfectos de La Manipulacion Esteopatica en El Desrden General de AnsiedadRafael MendietaPas encore d'évaluation
- 1203 FullDocument10 pages1203 FullMePas encore d'évaluation
- A Longitudinal Follow-Up Study of Anti-Depressant Drugs Causing Hepatotoxicity in Patients With Major Depressive DisordersDocument4 pagesA Longitudinal Follow-Up Study of Anti-Depressant Drugs Causing Hepatotoxicity in Patients With Major Depressive DisordersAbdul SamadPas encore d'évaluation
- Exercise Training and Music Therapy in Elderly With Depressive Syndrome: A Pilot StudyDocument7 pagesExercise Training and Music Therapy in Elderly With Depressive Syndrome: A Pilot StudymerawatidyahsepitaPas encore d'évaluation
- Topical Review ArticleDocument12 pagesTopical Review ArticleadnanjivrakPas encore d'évaluation
- Herbal - Medicines - in - The - Treatment of Mental IllnessesDocument12 pagesHerbal - Medicines - in - The - Treatment of Mental IllnessesFarash farshiPas encore d'évaluation
- BMC Psychiatry: Thyroid Function in Clinical Subtypes of Major Depression: An Exploratory StudyDocument9 pagesBMC Psychiatry: Thyroid Function in Clinical Subtypes of Major Depression: An Exploratory StudyTRTETDX TETDPas encore d'évaluation
- Nihms 1562854Document17 pagesNihms 1562854joseph psychayterPas encore d'évaluation
- Inflammation and Late-Life Depression: Unraveling The Complex Relationship and Potential Therapeutic StrategiesDocument18 pagesInflammation and Late-Life Depression: Unraveling The Complex Relationship and Potential Therapeutic Strategiesmustafa566512345Pas encore d'évaluation
- Acu 2012 0900Document9 pagesAcu 2012 0900pink bamasaqPas encore d'évaluation
- Adaptogenic and Anxiolytic Effects of AshwagandhaDocument13 pagesAdaptogenic and Anxiolytic Effects of AshwagandhaMuhammad UmerPas encore d'évaluation
- Bsico em Fitoterapia Chinesa Apostila03 PDFDocument8 pagesBsico em Fitoterapia Chinesa Apostila03 PDFAn MoraesPas encore d'évaluation
- Major Depressive DisorderDocument7 pagesMajor Depressive DisorderAbu SumayyahPas encore d'évaluation
- Ijerph 20 01555 v2Document16 pagesIjerph 20 01555 v2Diana DionisioPas encore d'évaluation
- Application of Antidepressants in Depression. A Systematic Review and Meta-AnalysisDocument14 pagesApplication of Antidepressants in Depression. A Systematic Review and Meta-AnalysisCésar Vásquez CohelloPas encore d'évaluation
- Sinta 5 - TERAPI TERTAWA MENURUNKAN DEPRESI PADA PERAWATAN - September 2021-DikonversiDocument10 pagesSinta 5 - TERAPI TERTAWA MENURUNKAN DEPRESI PADA PERAWATAN - September 2021-DikonversiAsnidarPas encore d'évaluation
- The Effectiveness of Acupressure On Severity of Depression in Hemodialysis Patients: A Randomized Controlled TrialDocument8 pagesThe Effectiveness of Acupressure On Severity of Depression in Hemodialysis Patients: A Randomized Controlled TrialpangaribuansantaPas encore d'évaluation
- P76 Depression AnnIntMed 2007Document16 pagesP76 Depression AnnIntMed 2007Gabriel CampolinaPas encore d'évaluation
- Development and Validation of Stability Indicating Assay Method For Estimation of Teriflunomide in Tablet Dosage FormDocument11 pagesDevelopment and Validation of Stability Indicating Assay Method For Estimation of Teriflunomide in Tablet Dosage FormBaru Chandrasekhar RaoPas encore d'évaluation
- Genetic Enhancment of Groundnut (Arachis Hypogaea L.) Through Induced Muiation.Document5 pagesGenetic Enhancment of Groundnut (Arachis Hypogaea L.) Through Induced Muiation.Baru Chandrasekhar RaoPas encore d'évaluation
- Knowledge On Antibiotics Use and Its Storage Among Saudi Arabia Residents: A Cross Sectional StudyDocument8 pagesKnowledge On Antibiotics Use and Its Storage Among Saudi Arabia Residents: A Cross Sectional StudyBaru Chandrasekhar RaoPas encore d'évaluation
- Simultaneous Estimation of Rosuvastatin Calcium and Ezetimibe As Bulk Drug and in Tablet Dosage Form by RP-HPLC MethodDocument6 pagesSimultaneous Estimation of Rosuvastatin Calcium and Ezetimibe As Bulk Drug and in Tablet Dosage Form by RP-HPLC MethodBaru Chandrasekhar RaoPas encore d'évaluation
- Analytical Method Development and Validation of Stability Indicating RP-HPLC Method For Estimation of Lercanidipine Hydrochloride and Enalapril Maleate in CombinationDocument8 pagesAnalytical Method Development and Validation of Stability Indicating RP-HPLC Method For Estimation of Lercanidipine Hydrochloride and Enalapril Maleate in CombinationBaru Chandrasekhar RaoPas encore d'évaluation
- Development of Cell Culture System From Selected Tissues of Pangaius HypopthalmusDocument6 pagesDevelopment of Cell Culture System From Selected Tissues of Pangaius HypopthalmusBaru Chandrasekhar RaoPas encore d'évaluation
- Formulation, Optimization and Evaluation Colon Targated Drug Delivery System For OrniadazoleDocument9 pagesFormulation, Optimization and Evaluation Colon Targated Drug Delivery System For OrniadazoleBaru Chandrasekhar RaoPas encore d'évaluation
- Gastroprotective Activity of Methanolic Extract of Phyllanthus Acidus Fruit Against Indomethacin-Induced Gastric Ulcers in RatsDocument7 pagesGastroprotective Activity of Methanolic Extract of Phyllanthus Acidus Fruit Against Indomethacin-Induced Gastric Ulcers in RatsBaru Chandrasekhar RaoPas encore d'évaluation
- Non-Adherence in Hyppertensive Patients of Peshawar, PakistanDocument13 pagesNon-Adherence in Hyppertensive Patients of Peshawar, PakistanBaru Chandrasekhar RaoPas encore d'évaluation
- The Bordering Areas (Nine Areas of Panjgur District) Issue of Pakistan About Human Malaria Prevalence: A Cross-Sectional Research of Malaria Parasites Identification in Blood SlidesDocument8 pagesThe Bordering Areas (Nine Areas of Panjgur District) Issue of Pakistan About Human Malaria Prevalence: A Cross-Sectional Research of Malaria Parasites Identification in Blood SlidesBaru Chandrasekhar RaoPas encore d'évaluation
- Preparation of Silver Nanoparticles From Herbal PlantDocument9 pagesPreparation of Silver Nanoparticles From Herbal PlantBaru Chandrasekhar RaoPas encore d'évaluation
- Nephroprotective Activityof Acorus Calamus Leaves Extract Against Lithium Induced Nephrotoxicity in Wistar RatsDocument12 pagesNephroprotective Activityof Acorus Calamus Leaves Extract Against Lithium Induced Nephrotoxicity in Wistar RatsBaru Chandrasekhar RaoPas encore d'évaluation
- A Brief Review On YawsDocument7 pagesA Brief Review On YawsBaru Chandrasekhar RaoPas encore d'évaluation
- Role of Simvastatin in Addition To Metformin in Polycystic Ovarian Syndrome Patients, A Randomized Controlled Trial On Pakistani WomenDocument4 pagesRole of Simvastatin in Addition To Metformin in Polycystic Ovarian Syndrome Patients, A Randomized Controlled Trial On Pakistani WomenBaru Chandrasekhar RaoPas encore d'évaluation
- Association of Socioeconomic Status, Hypertension and Treatment Modality With Diabetic Amputation - A Case Control StudyDocument4 pagesAssociation of Socioeconomic Status, Hypertension and Treatment Modality With Diabetic Amputation - A Case Control StudyBaru Chandrasekhar RaoPas encore d'évaluation
- Review On: Inventory ManagementDocument8 pagesReview On: Inventory ManagementBaru Chandrasekhar RaoPas encore d'évaluation
- Relationship of Testosterone With Body Mass Index in Infertile Males in Local CommunityDocument4 pagesRelationship of Testosterone With Body Mass Index in Infertile Males in Local CommunityBaru Chandrasekhar RaoPas encore d'évaluation
- Assessment of Correlation Between Physical Activity and Academic Performance Among The Students of Gujranwala Medical College, GujranwalaDocument7 pagesAssessment of Correlation Between Physical Activity and Academic Performance Among The Students of Gujranwala Medical College, GujranwalaBaru Chandrasekhar RaoPas encore d'évaluation
- An Exploratory Review of The Myths and Common Beliefs About Acne and Its TreatmentDocument6 pagesAn Exploratory Review of The Myths and Common Beliefs About Acne and Its TreatmentBaru Chandrasekhar RaoPas encore d'évaluation
- An Incidence of Hypertension Among People and Its Association To Consumption of Hard Water: A Cross-Sectional ResearchDocument6 pagesAn Incidence of Hypertension Among People and Its Association To Consumption of Hard Water: A Cross-Sectional ResearchBaru Chandrasekhar RaoPas encore d'évaluation
- Pharmaceutical Sciences: IAJPS 2018, 05 (04), 3075-3081 Aneeqa Ali RaoDocument7 pagesPharmaceutical Sciences: IAJPS 2018, 05 (04), 3075-3081 Aneeqa Ali RaoBaru Chandrasekhar RaoPas encore d'évaluation
- C-Reactive Protein Levels Preoperatively and Postoperatively Effect On Cardiovascular Surgery ComplicationsDocument5 pagesC-Reactive Protein Levels Preoperatively and Postoperatively Effect On Cardiovascular Surgery ComplicationsBaru Chandrasekhar RaoPas encore d'évaluation
- Descriptive Study Knowing The Patients Load in The Neonatal Icu at The Tertiary Care Hospital LahoreDocument4 pagesDescriptive Study Knowing The Patients Load in The Neonatal Icu at The Tertiary Care Hospital LahoreBaru Chandrasekhar RaoPas encore d'évaluation
- Isolation and Identification of Clostridium Perfringens Causing Enterotoxaemia in Bovine of Kacchi District Balochistan.Document8 pagesIsolation and Identification of Clostridium Perfringens Causing Enterotoxaemia in Bovine of Kacchi District Balochistan.Baru Chandrasekhar RaoPas encore d'évaluation
- After Acute Myocardial Infarction End Result of Cardiogenic Shock in Hospitalized PatientsDocument4 pagesAfter Acute Myocardial Infarction End Result of Cardiogenic Shock in Hospitalized PatientsBaru Chandrasekhar RaoPas encore d'évaluation
- A Cross Sectional Survey Information About Weaning Process Among Mothers of Infants Above 6 Months of Age in Opd Pediatrics at Kishwer Fazal Teaching Hospital LahoreDocument8 pagesA Cross Sectional Survey Information About Weaning Process Among Mothers of Infants Above 6 Months of Age in Opd Pediatrics at Kishwer Fazal Teaching Hospital LahoreBaru Chandrasekhar RaoPas encore d'évaluation
- An Epidemiological Survey About The Infections Caused by Dengue in The Perspective of Hematological, Clinical and Demographic Risk FactorsDocument6 pagesAn Epidemiological Survey About The Infections Caused by Dengue in The Perspective of Hematological, Clinical and Demographic Risk FactorsBaru Chandrasekhar RaoPas encore d'évaluation
- Study of Clinical Profile of Transfused Thalassemic Childrens With Special Reference To Hepatitis B Profile and Liver Function.Document6 pagesStudy of Clinical Profile of Transfused Thalassemic Childrens With Special Reference To Hepatitis B Profile and Liver Function.Baru Chandrasekhar RaoPas encore d'évaluation
- The Role of Clinical Pharmacist in Pharmacovigilance and Drug Safety in Teritiary Care Teaching HospitalDocument11 pagesThe Role of Clinical Pharmacist in Pharmacovigilance and Drug Safety in Teritiary Care Teaching HospitalBaru Chandrasekhar RaoPas encore d'évaluation
- Oppertunistic Hypertension Screening in Rural Health Population of Umar Abad Tehsil Kharezat Disrtrict Pishin Balochistan. A Cross Sectional StudyDocument10 pagesOppertunistic Hypertension Screening in Rural Health Population of Umar Abad Tehsil Kharezat Disrtrict Pishin Balochistan. A Cross Sectional StudyBaru Chandrasekhar RaoPas encore d'évaluation
- NCM 104 Cellular Aberration Lecture 2007Document104 pagesNCM 104 Cellular Aberration Lecture 2007Keith Gulmatico Fantinalgo67% (3)
- CH 29Document39 pagesCH 29Jann Zaniel Allayne RiPas encore d'évaluation
- June 2018 QP - Paper 2 AQA Biology A-LevelDocument32 pagesJune 2018 QP - Paper 2 AQA Biology A-LevelreneehandsPas encore d'évaluation
- CELL PathologyDocument28 pagesCELL PathologySaeed RazaqPas encore d'évaluation
- Biochip Project ReportDocument21 pagesBiochip Project ReportAjay Ranga100% (1)
- Moringa OleiferaDocument4 pagesMoringa Oleiferajap pagharionPas encore d'évaluation
- Don Juans, Monks, and Multi-Orgasmic WormsDocument1 pageDon Juans, Monks, and Multi-Orgasmic WormskukutxiPas encore d'évaluation
- (TS) Incoming SR Elite & Aiims s60 Neet Weekend Test - 8 Paper (05!10!2021)Document22 pages(TS) Incoming SR Elite & Aiims s60 Neet Weekend Test - 8 Paper (05!10!2021)Alle ArunkumarPas encore d'évaluation
- AlopeciaDocument10 pagesAlopeciaDr Vaishali MathapatiPas encore d'évaluation
- Autoimmune Bullous Dermatoses - Overview of Serological Diagnostics in Blister Forming Diseases of The SkinDocument8 pagesAutoimmune Bullous Dermatoses - Overview of Serological Diagnostics in Blister Forming Diseases of The SkinFedoxyzPas encore d'évaluation
- Case PresentationDocument21 pagesCase PresentationMae Alleslie TolentinoPas encore d'évaluation
- Somatoform Disorder - DR - Ziad Arandi PowerpointDocument40 pagesSomatoform Disorder - DR - Ziad Arandi PowerpointNaji Z. ArandiPas encore d'évaluation
- TRP-C5 Sensor Odontoblastos FrioDocument13 pagesTRP-C5 Sensor Odontoblastos FrioIgna Sarquis AbumohorPas encore d'évaluation
- What Is A Bladder Diverticulum?Document3 pagesWhat Is A Bladder Diverticulum?luckyariadneePas encore d'évaluation
- Dynamics of Tooth MovementDocument80 pagesDynamics of Tooth Movementdentistpro.orgPas encore d'évaluation
- Bone HealingDocument2 pagesBone HealingGerardLum100% (2)
- Testicular CancerDocument24 pagesTesticular CancerJulianne LeePas encore d'évaluation
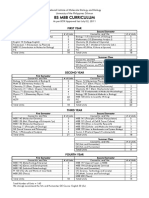
- UG BS Curriculum UpdatedDocument2 pagesUG BS Curriculum UpdatedyayPas encore d'évaluation
- Care of Clients With Problems in Cellular Aberration, Acute and ChronicDocument5 pagesCare of Clients With Problems in Cellular Aberration, Acute and ChronicRika Mae DiamosPas encore d'évaluation
- Hybridoma TechnologyDocument16 pagesHybridoma TechnologyDhanush BharadwajPas encore d'évaluation
- Kayatsha - Gastroschisis and Omphalocele A Case ReportDocument4 pagesKayatsha - Gastroschisis and Omphalocele A Case ReportAffannul HakimPas encore d'évaluation
- Small Round Cell Tumors of Soft Tissue and BoneDocument13 pagesSmall Round Cell Tumors of Soft Tissue and BoneAdriana Gabriela Ugarte MacíasPas encore d'évaluation
- Diabetes Advances in Diagnosis and TreatmentDocument11 pagesDiabetes Advances in Diagnosis and TreatmentAbi GarciaPas encore d'évaluation
- SOPDocument2 pagesSOPNIGEL SAANAPas encore d'évaluation
- NCBI ResourcesDocument13 pagesNCBI ResourceshamzaloPas encore d'évaluation
- Medical E Book TitlesApril 2017Document35 pagesMedical E Book TitlesApril 2017kevin CTPas encore d'évaluation
- Array FlipbookDocument40 pagesArray FlipbookSanja CirkovicPas encore d'évaluation
- Legal MedDocument2 pagesLegal MedHanna Supetran0% (1)
- Inserto Vitamina B12 CTKDocument2 pagesInserto Vitamina B12 CTKLilian Carolina Loreto MachadoPas encore d'évaluation
- HemoglobinDocument15 pagesHemoglobinArya RaoPas encore d'évaluation