Vous aimerez peut-être aussi
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Ijerph 16 03937Document14 pagesIjerph 16 03937anggaririnPas encore d'évaluation
- BPJ 41 Cephalosporins Pages 22-28Document7 pagesBPJ 41 Cephalosporins Pages 22-28anggaririnPas encore d'évaluation
- Harrison 2008Document12 pagesHarrison 2008anggaririnPas encore d'évaluation
- Cephalosporins Pharmacology and ChemistryDocument5 pagesCephalosporins Pharmacology and ChemistryIrfan QaisarPas encore d'évaluation
- Betalaktamase Di SefalosporinDocument10 pagesBetalaktamase Di SefalosporinAlfauzanSaputraPas encore d'évaluation
- Kumar 2017Document31 pagesKumar 2017anggaririnPas encore d'évaluation
- The New Fifth-Generation Cephalosporins - A BalancDocument7 pagesThe New Fifth-Generation Cephalosporins - A BalancanggaririnPas encore d'évaluation
- Quino LoneDocument28 pagesQuino LoneanggaririnPas encore d'évaluation
- Immunological Memory To SARS-CoV-2 Assessed For Up To 8 Months After InfectionDocument15 pagesImmunological Memory To SARS-CoV-2 Assessed For Up To 8 Months After InfectionChevy LuvianaPas encore d'évaluation
- MonkeyfoxDocument20 pagesMonkeyfoxanggaririnPas encore d'évaluation
- Nej Mo A 2118691Document14 pagesNej Mo A 2118691anggaririnPas encore d'évaluation
- Pi Is 1473309921006769Document3 pagesPi Is 1473309921006769PDFReadAndDevelopPas encore d'évaluation
- Jama Abbasi 2021 MN 210043 1627852635.57854Document2 pagesJama Abbasi 2021 MN 210043 1627852635.57854anggaririnPas encore d'évaluation
- Mechanisms Efflux Pumps of Acinetobacter To Antibiotics: Baumannii (MDR) : Increasing ResistanceDocument23 pagesMechanisms Efflux Pumps of Acinetobacter To Antibiotics: Baumannii (MDR) : Increasing ResistanceanggaririnPas encore d'évaluation
- Hiv WhoDocument480 pagesHiv Whoأبو أويس شرف الدينPas encore d'évaluation
- Pi Is 1473309922002286Document10 pagesPi Is 1473309922002286anggaririnPas encore d'évaluation
- Comparison of Commensal and Clinical Isolates For Diversity PDFDocument8 pagesComparison of Commensal and Clinical Isolates For Diversity PDFanggaririnPas encore d'évaluation
- Molecular Mechanisms of Antibiotic Resistance PDFDocument7 pagesMolecular Mechanisms of Antibiotic Resistance PDFanggaririnPas encore d'évaluation
- The Diagnostic Use of ADVIA 2120i Siemens and An "APL Criteria" CanDocument9 pagesThe Diagnostic Use of ADVIA 2120i Siemens and An "APL Criteria" CananggaririnPas encore d'évaluation
- Genetic Diversity of Carbapenem-Resistant Enterobacteriaceae (CRE) Clinical Isolates From A Tertiary Hospital in Eastern China PDFDocument8 pagesGenetic Diversity of Carbapenem-Resistant Enterobacteriaceae (CRE) Clinical Isolates From A Tertiary Hospital in Eastern China PDFanggaririnPas encore d'évaluation
- Kirchhoff HIV Life CycleDocument10 pagesKirchhoff HIV Life CycleanggaririnPas encore d'évaluation
- Hepcidine N Iron Metabolisme PDFDocument23 pagesHepcidine N Iron Metabolisme PDFanggaririnPas encore d'évaluation
- Chapter 2Document34 pagesChapter 2Anonymous 1EQutBPas encore d'évaluation
- Association of High-Sensitivity Cardiac PDFDocument9 pagesAssociation of High-Sensitivity Cardiac PDFanggaririnPas encore d'évaluation
- Association Between Early Systemic Inflammatory Response, Severity of Multiorgan Dysfunction and Death in Acute PancreatitisDocument7 pagesAssociation Between Early Systemic Inflammatory Response, Severity of Multiorgan Dysfunction and Death in Acute PancreatitisanggaririnPas encore d'évaluation
- BiomarkerDocument18 pagesBiomarkeranggaririnPas encore d'évaluation
- CD200 Is A Useful Diagnostic Marker For Identifying AtypicalDocument7 pagesCD200 Is A Useful Diagnostic Marker For Identifying AtypicalanggaririnPas encore d'évaluation
- Patogenesis Bone Disease Di MMDocument12 pagesPatogenesis Bone Disease Di MManggaririnPas encore d'évaluation
- Comparative Study of Four Fluorescent Probes For Evaluation of NaturalDocument12 pagesComparative Study of Four Fluorescent Probes For Evaluation of NaturalanggaririnPas encore d'évaluation
- Shiv N Mucosal IgG N IgADocument7 pagesShiv N Mucosal IgG N IgAanggaririnPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Jurnal 1Document14 pagesJurnal 1Winona ProkPas encore d'évaluation
- Short Story Ibrahim SomethingDocument29 pagesShort Story Ibrahim SomethingNABUDAKZPas encore d'évaluation
- Peter Lee Story PRESS KefaloniaDocument2 pagesPeter Lee Story PRESS KefaloniaAnonymous Drqem9zxJPas encore d'évaluation
- Alisha ResumeDocument2 pagesAlisha ResumePaul R BurklowPas encore d'évaluation
- Unit Test 2BDocument2 pagesUnit Test 2BSantiago Contreras0% (1)
- Post-Seclusion And/or Restraint Review in Psychiatry: A Scoping Review Article OutlineDocument27 pagesPost-Seclusion And/or Restraint Review in Psychiatry: A Scoping Review Article OutlineStudentnurseMjPas encore d'évaluation
- Nurs 401s ResumeDocument3 pagesNurs 401s Resumeapi-347598554Pas encore d'évaluation
- Ida Jean OrlandoDocument5 pagesIda Jean OrlandoZhij Constante100% (1)
- Distraction and Coping TechniquesDocument14 pagesDistraction and Coping TechniquesSiva KumarrPas encore d'évaluation
- NCM 110 Lec Nursing Informatics Technology Part 1Document5 pagesNCM 110 Lec Nursing Informatics Technology Part 1Krizle Adaza0% (1)
- Handbook of Pain ManagementDocument730 pagesHandbook of Pain Managementanon_990504998100% (6)
- Essentials of ProsthodonticsDocument215 pagesEssentials of ProsthodonticsGenesis Centeno100% (5)
- MST Nursing HandoutDocument3 pagesMST Nursing Handoutapi-261265221Pas encore d'évaluation
- A Questionnaire Survey On Attitudes and Understanding Towards Mental DisordersDocument7 pagesA Questionnaire Survey On Attitudes and Understanding Towards Mental DisordersDedah IssaPas encore d'évaluation
- Clinical PortraitDocument6 pagesClinical PortraitDann Francis SarnilloPas encore d'évaluation
- Care of Ventilated PatientsDocument2 pagesCare of Ventilated PatientsRaydan Francis Magana Antojado100% (1)
- Pharmacy ManualDocument54 pagesPharmacy ManualAmir Ramadan100% (2)
- Hamida Haron CaseDocument5 pagesHamida Haron CasegadzPas encore d'évaluation
- Benefits of The Costoclavicular Space For.15Document2 pagesBenefits of The Costoclavicular Space For.15andrew herringPas encore d'évaluation
- English Drama Script in The HospitalDocument4 pagesEnglish Drama Script in The HospitalS Yogaa Muliaa100% (1)
- Facility Planning TemplateDocument4 pagesFacility Planning TemplateJohn Troy GamilPas encore d'évaluation
- Gymnastics - Artistic Gymnastics: Sport Technical ManualDocument28 pagesGymnastics - Artistic Gymnastics: Sport Technical ManualCharles MercadoPas encore d'évaluation
- Carla Yanni The Architecture of Madness Insane Asylums in The United States Architecture Landscape and Amer Culture 2007Document206 pagesCarla Yanni The Architecture of Madness Insane Asylums in The United States Architecture Landscape and Amer Culture 2007Joana Melo Resende100% (3)
- Causes and Treatment Outcome of Mechanical Bowel Obstruction in North Eastern NigeriaDocument3 pagesCauses and Treatment Outcome of Mechanical Bowel Obstruction in North Eastern NigeriakeithPas encore d'évaluation
- Kasus 3 KardiovaskularDocument3 pagesKasus 3 KardiovaskularHelmin DhPas encore d'évaluation
- Comunicare Lb. Engleza DialogDocument3 pagesComunicare Lb. Engleza DialogLaurus AdiaPas encore d'évaluation
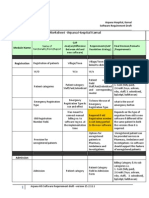
- Finalized Requirements-Worksheet - Arpana Hospital KarnalDocument11 pagesFinalized Requirements-Worksheet - Arpana Hospital KarnalMahesh PatilPas encore d'évaluation
- Role of Amo in Pre Hospital Care andDocument20 pagesRole of Amo in Pre Hospital Care andWan AmeeramirulzamanPas encore d'évaluation
- Railway Concession CertificateDocument1 pageRailway Concession Certificatekumar130976% (17)
- Strategies To Prevent Central Line-Associated Bloodstream Infections in Acute Care - 1836 - 21-07-13-15-29-36Document20 pagesStrategies To Prevent Central Line-Associated Bloodstream Infections in Acute Care - 1836 - 21-07-13-15-29-36Marcela Rios HernandezPas encore d'évaluation