Vous aimerez peut-être aussi
- Introduction To How To Use GRADE: Time Topic SpeakerDocument1 pageIntroduction To How To Use GRADE: Time Topic SpeakerirsalinahusnaPas encore d'évaluation
- 10 1016@j Jaad 2013 01 032Document9 pages10 1016@j Jaad 2013 01 032irsalinahusnaPas encore d'évaluation
- Brosur Deka Pigmented LaserDocument4 pagesBrosur Deka Pigmented LaserirsalinahusnaPas encore d'évaluation
- 1475 2875 11 39 PDFDocument11 pages1475 2875 11 39 PDFirsalinahusnaPas encore d'évaluation
- Reconstruction After Skin Cancer Removal: More Than Just "Filling A Hole"Document2 pagesReconstruction After Skin Cancer Removal: More Than Just "Filling A Hole"irsalinahusnaPas encore d'évaluation
- Pemphigus Vulgaris Complicated by Pregnancy: Thomas W. Mcelin, M.D. M.S. David W. Cromer, M.DDocument1 pagePemphigus Vulgaris Complicated by Pregnancy: Thomas W. Mcelin, M.D. M.S. David W. Cromer, M.DirsalinahusnaPas encore d'évaluation
- Cellular DefectsDocument33 pagesCellular DefectsirsalinahusnaPas encore d'évaluation
- Continous Vs Be Going ToDocument2 pagesContinous Vs Be Going ToirsalinahusnaPas encore d'évaluation
- VitiligoDocument13 pagesVitiligoFebyan AbotPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- My ResumeDocument3 pagesMy ResumeKc Velle Pagangpang ReginaldoPas encore d'évaluation
- IELTS Writing Task 1 - Describing Table.Document12 pagesIELTS Writing Task 1 - Describing Table.Mohamadreza JafaryPas encore d'évaluation
- The Reaction Paper, Review, and CritiqueDocument16 pagesThe Reaction Paper, Review, and CritiqueChristian PapaPas encore d'évaluation
- Managing A Successful Computing ProjectDocument20 pagesManaging A Successful Computing ProjectAryan AmatyaPas encore d'évaluation
- Analysing A Sample LSA (Skills) BEDocument23 pagesAnalysing A Sample LSA (Skills) BECPPE ARTEPas encore d'évaluation
- Swift Training Swiftsmart Full Training Catalogue December 2016Document15 pagesSwift Training Swiftsmart Full Training Catalogue December 2016Oscar Alberto ZambranoPas encore d'évaluation
- Modified Double Glove TechniqueDocument1 pageModified Double Glove TechniqueSohaib NawazPas encore d'évaluation
- Performancce TaskDocument5 pagesPerformancce Taskapi-638308201Pas encore d'évaluation
- Kellogg Employment Report 2020Document24 pagesKellogg Employment Report 2020Keerthana RaoPas encore d'évaluation
- Private Form Latest - 2015Document16 pagesPrivate Form Latest - 2015ksachdeva23Pas encore d'évaluation
- Classroom Assessments Checklists, Rating Scales, and RubricsDocument24 pagesClassroom Assessments Checklists, Rating Scales, and RubricsJoseph Ajayi FAYOMIPas encore d'évaluation
- Ethics Report GRP 3Document3 pagesEthics Report GRP 3MikaPas encore d'évaluation
- Relative Clauses Grammar ReferenceDocument2 pagesRelative Clauses Grammar ReferencemariecbaPas encore d'évaluation
- WFA Competency LevelsDocument5 pagesWFA Competency LevelsTroy Lyons DunowPas encore d'évaluation
- Feral and Stray Cats - An Important Difference: BehaviorDocument4 pagesFeral and Stray Cats - An Important Difference: BehaviorVinayak RaoPas encore d'évaluation
- Actividad Entregable 2 - RoutinesDocument3 pagesActividad Entregable 2 - RoutinesAnggie ApoloPas encore d'évaluation
- The Epistles of St. Paul Written After He Became A Prisoner Boise, James Robinson, 1815-1895Document274 pagesThe Epistles of St. Paul Written After He Became A Prisoner Boise, James Robinson, 1815-1895David BaileyPas encore d'évaluation
- Ya Literature Past and PresentDocument10 pagesYa Literature Past and Presentapi-296864651Pas encore d'évaluation
- Why Women Wash DishesDocument9 pagesWhy Women Wash Dishesmoodswingss100% (1)
- Colegio de Calumpit Inc.: Iba O' Este, Calumpit, BulacanDocument1 pageColegio de Calumpit Inc.: Iba O' Este, Calumpit, BulacanJessie AndreiPas encore d'évaluation
- Air-in-Line Alarms: Decreasing Alarms Through Antisiphon Valve ImplementationDocument3 pagesAir-in-Line Alarms: Decreasing Alarms Through Antisiphon Valve ImplementationSjis11362Pas encore d'évaluation
- Reconstruct Lesson Plan - Polynomials - BinoyaDocument9 pagesReconstruct Lesson Plan - Polynomials - BinoyaRICHARD BINOYAPas encore d'évaluation
- Literature Review of Pick and Place RobotDocument4 pagesLiterature Review of Pick and Place Robotgvzf446w100% (1)
- ww2 PFTDocument15 pagesww2 PFTLPicarodaPas encore d'évaluation
- 1 Full List of LkoDocument6 pages1 Full List of Lkomohd yusuf ansariPas encore d'évaluation
- SBM VAlidation FormDocument2 pagesSBM VAlidation FormamerizaPas encore d'évaluation
- YeshivishDocument5 pagesYeshivishdzimmer6Pas encore d'évaluation
- Practical ResearchDocument33 pagesPractical ResearchMonica SibayanPas encore d'évaluation
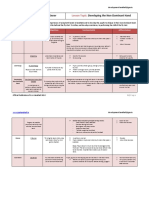
- Lesson 4 - Developing The Non-Dominant HandDocument6 pagesLesson 4 - Developing The Non-Dominant HandBlaja AroraArwen AlexisPas encore d'évaluation
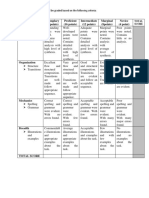
- 20 Points RubricsDocument1 page20 Points RubricsJerome Formalejo,Pas encore d'évaluation