Vous aimerez peut-être aussi
- Dermatology Notes for Medical StudentsD'EverandDermatology Notes for Medical StudentsÉvaluation : 4 sur 5 étoiles4/5 (5)
- Pemicu 2 "Ada Apa Dengan Mataku?": Adrian Pratama - 405100018 - Blok PenginderaanDocument82 pagesPemicu 2 "Ada Apa Dengan Mataku?": Adrian Pratama - 405100018 - Blok PenginderaanRilianda SimbolonPas encore d'évaluation
- Eye Infection /inflammation: Presented byDocument49 pagesEye Infection /inflammation: Presented byPriya bhattiPas encore d'évaluation
- Ophthalmology - Diseases of The EyelidsDocument9 pagesOphthalmology - Diseases of The EyelidsjbtcmdtjjvPas encore d'évaluation
- Eye Adnexa Diseases: Catedra OftalmologieDocument39 pagesEye Adnexa Diseases: Catedra OftalmologieDanielaPas encore d'évaluation
- Skin and Soft Tissue Infectons 1Document51 pagesSkin and Soft Tissue Infectons 1AISHWARYA T DPas encore d'évaluation
- Kuliah Blok Mata: Halida Wibawaty Infection Immunology Subdivision Department of Ophthalmology RSUD DR Moewardi SurakartaDocument51 pagesKuliah Blok Mata: Halida Wibawaty Infection Immunology Subdivision Department of Ophthalmology RSUD DR Moewardi SurakartaMuhammad Nur SidiqPas encore d'évaluation
- Preceptor: Dr. Rahmat Syuhada SP.M (K) : BlefaritisDocument23 pagesPreceptor: Dr. Rahmat Syuhada SP.M (K) : BlefaritisAndre BinsarPas encore d'évaluation
- Kuliah Mata Merah, Kelainan Struktur Dan Bentuk Mata - DR NaziyaDocument47 pagesKuliah Mata Merah, Kelainan Struktur Dan Bentuk Mata - DR NaziyaFastiati RAPas encore d'évaluation
- P ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Document48 pagesP ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Nauli PanjaitanPas encore d'évaluation
- Dr. Mubashir Rehman: Assistant ProfessorDocument112 pagesDr. Mubashir Rehman: Assistant Professorsaqibullah gulPas encore d'évaluation
- Eyelid Disorders: Hordeolum, Chalazion, Blepharitis, TrichiasisDocument19 pagesEyelid Disorders: Hordeolum, Chalazion, Blepharitis, TrichiasisWulan NeenPas encore d'évaluation
- Baterial & Fungal Corneal UlcersDocument28 pagesBaterial & Fungal Corneal UlcersVasishta NadellaPas encore d'évaluation
- 789 Baterial and Fungal Corneal UlcersDocument28 pages789 Baterial and Fungal Corneal UlcersMounika PapireddyPas encore d'évaluation
- Bacterial ConjunctivitisDocument5 pagesBacterial ConjunctivitisBnB UsmlePas encore d'évaluation
- Diskusi Topik BlepharitisDocument10 pagesDiskusi Topik BlepharitisDwi Permana PutraPas encore d'évaluation
- Disease of Orbit, LacrimalDocument73 pagesDisease of Orbit, LacrimalMarshet GetePas encore d'évaluation
- The Cornea PPT EditDocument38 pagesThe Cornea PPT EditRahman Setiawan100% (1)
- Disease of Lids and Lacrim Al Apparatus: The First Affiliated Hospital of Zhengzhou UniversityDocument46 pagesDisease of Lids and Lacrim Al Apparatus: The First Affiliated Hospital of Zhengzhou Universityapi-19916399Pas encore d'évaluation
- Microbial Keratitis: Causes, Symptoms, Signs and ManagementDocument56 pagesMicrobial Keratitis: Causes, Symptoms, Signs and ManagementRanveerPas encore d'évaluation
- Disorders of The Eye LidsDocument33 pagesDisorders of The Eye Lidsc/risaaq yuusuf ColoowPas encore d'évaluation
- Pyodermas 2014Document41 pagesPyodermas 2014Dudy Humaedi100% (6)
- Diseases of Eyelid: Prepared by DR - Sourab Kumar DasDocument66 pagesDiseases of Eyelid: Prepared by DR - Sourab Kumar Dasসপ্নে ছোয়া মনPas encore d'évaluation
- Kelainan Kelopak Mata DKKDocument28 pagesKelainan Kelopak Mata DKKbinto akturusianoPas encore d'évaluation
- Conjunctiva Anatomy and Physiology NewDocument78 pagesConjunctiva Anatomy and Physiology Newfachrie saputraPas encore d'évaluation
- ConjunctivitisDocument27 pagesConjunctivitisGAURAVPas encore d'évaluation
- EedDocument70 pagesEedzihniyya471Pas encore d'évaluation
- Mata MerahDocument119 pagesMata MerahAzwanHamdiPas encore d'évaluation
- Conjunctival Diseases Presentation New Version SendDocument82 pagesConjunctival Diseases Presentation New Version Sendruhulcoc1Pas encore d'évaluation
- Bullous Disorders, Bacterial and Fungal Skin InfectionsDocument95 pagesBullous Disorders, Bacterial and Fungal Skin InfectionsDeborah ChemutaiPas encore d'évaluation
- Overview of Skin InfectionsDocument53 pagesOverview of Skin Infectionsadamu mohammadPas encore d'évaluation
- Inflammatory-Skin-Diseases 231101 174335 (2462)Document37 pagesInflammatory-Skin-Diseases 231101 174335 (2462)Moayad IsmailPas encore d'évaluation
- 1) Bacterial Skin InfDocument32 pages1) Bacterial Skin InfsmrutuPas encore d'évaluation
- finalPEDIATRIC DERMATOLOGYDocument58 pagesfinalPEDIATRIC DERMATOLOGYShiva RamPas encore d'évaluation
- PiodermaDocument43 pagesPiodermashlprtPas encore d'évaluation
- 2 EyelidsDocument18 pages2 Eyelidscawsey mohamedPas encore d'évaluation
- Treating Stye, Chalazion and TrichiasisDocument4 pagesTreating Stye, Chalazion and TrichiasishiPas encore d'évaluation
- Nor Hasyimah Binti Malek C11111885 Saidah Mafisah C11111315 Advisor: Dr. Suci Budiani SupervisorDocument20 pagesNor Hasyimah Binti Malek C11111885 Saidah Mafisah C11111315 Advisor: Dr. Suci Budiani SupervisorSyaidah MafisyahPas encore d'évaluation
- PYODERMA: Classification and Management of Common Pyodermas Including Impetigo, Folliculitis, Furuncle, Carbuncle, Echtyma, Paronikia, Erysipelas and Staphylococcal Scalded Skin SyndromeDocument43 pagesPYODERMA: Classification and Management of Common Pyodermas Including Impetigo, Folliculitis, Furuncle, Carbuncle, Echtyma, Paronikia, Erysipelas and Staphylococcal Scalded Skin SyndromeAnisaPas encore d'évaluation
- Conjunctiva Anatomy and PhysiologyDocument101 pagesConjunctiva Anatomy and PhysiologyPurva KeswaniPas encore d'évaluation
- Bacterial Keratitis PritiDocument58 pagesBacterial Keratitis Pritipriti08988% (8)
- Eyelids AdnexalDocument52 pagesEyelids AdnexalRushdaPas encore d'évaluation
- 2 - Ocularsurface2022Document76 pages2 - Ocularsurface2022MERAYM TRABLSIPas encore d'évaluation
- Common Ophthalmic DisordersDocument29 pagesCommon Ophthalmic DisordersSamirPas encore d'évaluation
- AK Khurana - Hordoleum KalazionDocument3 pagesAK Khurana - Hordoleum KalazionhiPas encore d'évaluation
- Inflammatory Disorders of The Eyelids: BlepharitisDocument3 pagesInflammatory Disorders of The Eyelids: BlepharitisNadia Indah AlvitaPas encore d'évaluation
- Gangguan Kelopak MataDocument88 pagesGangguan Kelopak MataraiPas encore d'évaluation
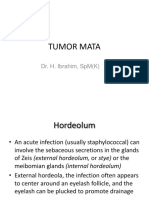
- Tumor Mata: Dr. H. Ibrahim, SPM (K)Document37 pagesTumor Mata: Dr. H. Ibrahim, SPM (K)vivilmPas encore d'évaluation
- Diseases of CorneaDocument170 pagesDiseases of CorneaLavanya MadabushiPas encore d'évaluation
- RED EYE WITH DECREASED VISION FixedDocument70 pagesRED EYE WITH DECREASED VISION FixedChandraPas encore d'évaluation
- ConjunctivaDocument40 pagesConjunctivaSarahPas encore d'évaluation
- Bacterial Infections of Oral CavityDocument63 pagesBacterial Infections of Oral CavityAkash Anilkumar Malini60% (5)
- 16-12-2014 Kuliah Pioderma - Dr. AsihDocument56 pages16-12-2014 Kuliah Pioderma - Dr. AsihSilvia SudjadiPas encore d'évaluation
- Blefaritis EarlyDocument28 pagesBlefaritis EarlyPaomo Zhixia EarlyPas encore d'évaluation
- InfectionDocument3 pagesInfectionAndrew BonusPas encore d'évaluation
- Penyakit Pada MataDocument138 pagesPenyakit Pada Matadevi taqiyyahPas encore d'évaluation
- Conjunctivita - PPT (Lb. Engleza)Document107 pagesConjunctivita - PPT (Lb. Engleza)Ciubotaru CristiPas encore d'évaluation
- Corneal Infections: HundumaDocument40 pagesCorneal Infections: HundumaHawwi IsmailPas encore d'évaluation
- Eyelid Disorders Guide: Ptosis, Blepharitis, Hordeolum & MoreDocument48 pagesEyelid Disorders Guide: Ptosis, Blepharitis, Hordeolum & MoreUdaif BabuPas encore d'évaluation
- Keratitis: Causes, Symptoms and TreatmentDocument28 pagesKeratitis: Causes, Symptoms and TreatmentjantyPas encore d'évaluation
- Early Preg Vaginal Microbiome Trends and Preterm BirthDocument18 pagesEarly Preg Vaginal Microbiome Trends and Preterm BirthNailul RosyidaPas encore d'évaluation
- Speaker:Dr - Ala' Abu Farsakh Supervised By:dr - Amjad YounisDocument67 pagesSpeaker:Dr - Ala' Abu Farsakh Supervised By:dr - Amjad YounisNailul RosyidaPas encore d'évaluation
- Adverse Preg, Birth, and Infant Outcomes in TwinsDocument15 pagesAdverse Preg, Birth, and Infant Outcomes in TwinsnanaPas encore d'évaluation
- A RCT of Foley Bulb For Labor Induction in PROMDocument7 pagesA RCT of Foley Bulb For Labor Induction in PROMNailul RosyidaPas encore d'évaluation
- A RCT of Foley Bulb For Labor Induction in PROMDocument7 pagesA RCT of Foley Bulb For Labor Induction in PROMNailul RosyidaPas encore d'évaluation
- Guide to Understanding BlepharitisDocument39 pagesGuide to Understanding BlepharitisNailul RosyidaPas encore d'évaluation
- Impact of USPSTF Recommendations For Aspirin For Prevention of Recurrent PreeclampsiaDocument8 pagesImpact of USPSTF Recommendations For Aspirin For Prevention of Recurrent PreeclampsiaNailul RosyidaPas encore d'évaluation
- Abdominal 20xray 20images 130628215452 Phpapp02Document53 pagesAbdominal 20xray 20images 130628215452 Phpapp02Nailul RosyidaPas encore d'évaluation
- DR Mohit Goel JR 11-05-2012Document51 pagesDR Mohit Goel JR 11-05-2012nailul rosyidaPas encore d'évaluation
- Learnultrasonography 170804145010Document105 pagesLearnultrasonography 170804145010Nailul RosyidaPas encore d'évaluation
- 13.10.10-Eyelid and Adnexal Disease 2, PPT Presentasi 23 Okt 2009Document51 pages13.10.10-Eyelid and Adnexal Disease 2, PPT Presentasi 23 Okt 2009Ronald Ariyanto Wiradirnata0% (1)
- Hordeolum PDFDocument2 pagesHordeolum PDFVan KochkarianPas encore d'évaluation
- Atlas of Clinical Ophthalmology 2nd Edition (2013)Document506 pagesAtlas of Clinical Ophthalmology 2nd Edition (2013)bogdasus75% (4)
- Hordeolum Guide: Causes, Symptoms and TreatmentDocument5 pagesHordeolum Guide: Causes, Symptoms and TreatmentLutfiaPutriBastianPas encore d'évaluation
- Red EyesDocument3 pagesRed EyesirijoaPas encore d'évaluation
- Common eye conditions managementDocument24 pagesCommon eye conditions managementexposus2003Pas encore d'évaluation
- Arsen Alb Arsen Alb. Belladona Hepar Sulph Nux Vom Pulsatilla Rhus Tox Silicea SulphurDocument10 pagesArsen Alb Arsen Alb. Belladona Hepar Sulph Nux Vom Pulsatilla Rhus Tox Silicea SulphurSouvik RoyPas encore d'évaluation
- Causes and Treatment of Red EyeDocument52 pagesCauses and Treatment of Red EyePatricia May CruzPas encore d'évaluation
- Chalazion and Hordeolum (Stye) - Eye Disorders - Merck Manuals Professional EditionDocument3 pagesChalazion and Hordeolum (Stye) - Eye Disorders - Merck Manuals Professional EditionAlfina MeidinaPas encore d'évaluation
- Anatomy of Human EyeDocument41 pagesAnatomy of Human EyeCarly MelachioPas encore d'évaluation
- Benign Eyelid Lesions: Identification and TreatmentDocument20 pagesBenign Eyelid Lesions: Identification and TreatmentShari' Si WahyuPas encore d'évaluation
- Peer Group Teachingon Eye DisordersDocument30 pagesPeer Group Teachingon Eye DisordersMary MenuPas encore d'évaluation
- Community Group AssignmentDocument8 pagesCommunity Group AssignmentClare EdralynnePas encore d'évaluation
- Red EyeDocument6 pagesRed EyeafatPas encore d'évaluation
- Pathophysiology: United StatesDocument11 pagesPathophysiology: United StatesNurullia RahmawatiPas encore d'évaluation
- Eye and Ear Disorders UpdatedDocument78 pagesEye and Ear Disorders Updatedjose arreolaPas encore d'évaluation
- 02 106學測英文試卷定稿Document8 pages02 106學測英文試卷定稿Chen LincolnPas encore d'évaluation
- StyesDocument3 pagesStyesRadya Andhika BagaskaraPas encore d'évaluation
- Eye InjuriesDocument3 pagesEye InjuriesSameera FernandoPas encore d'évaluation
- Contra-Indications: NVQ Level 2 Beauty TherapyDocument24 pagesContra-Indications: NVQ Level 2 Beauty TherapyUzma Khan100% (1)
- Palpebra Dan Jaringan Orbita FixDocument77 pagesPalpebra Dan Jaringan Orbita FixRiezqi Aditya Putra BakriPas encore d'évaluation
- NR 602 Final Exam Study GuideDocument113 pagesNR 602 Final Exam Study GuideAdam HenryPas encore d'évaluation
- Eye Infection and Blepharitis by MHSNDocument18 pagesEye Infection and Blepharitis by MHSNMhsn0% (1)
- Therapy LV CNS 4th Year KirubelDocument156 pagesTherapy LV CNS 4th Year Kirubelpblinder1319Pas encore d'évaluation
- MD PW 1,2 Eyelids and AnatomyDocument84 pagesMD PW 1,2 Eyelids and Anatomytaliya. shvetzPas encore d'évaluation
- Dr. Sadeli Masria, DR., SPMK., Ms. DMMDocument64 pagesDr. Sadeli Masria, DR., SPMK., Ms. DMMPraluki HerliawanPas encore d'évaluation
- Eyelid Tumor Diagnosis TreatmentDocument2 pagesEyelid Tumor Diagnosis TreatmentVera AvliwaniPas encore d'évaluation
- EYE DISORDERS GUIDEDocument115 pagesEYE DISORDERS GUIDEKwabena AmankwaPas encore d'évaluation
- Sure Success in Ophthalmology Viva Voce & Practical Examination - 2013 PDFDocument300 pagesSure Success in Ophthalmology Viva Voce & Practical Examination - 2013 PDFKaran Kumarswamy79% (14)
- Eye Disorder PeadsDocument51 pagesEye Disorder PeadsGrashiaPas encore d'évaluation