Vous aimerez peut-être aussi
- Nursing Study Guide: Your Nursing Assistant To Do Well In SchoolD'EverandNursing Study Guide: Your Nursing Assistant To Do Well In SchoolÉvaluation : 3 sur 5 étoiles3/5 (2)
- Nurses NotesDocument1 pageNurses Notesmona_javier100% (4)
- PT 2 Nurse NotesDocument1 pagePT 2 Nurse NotesAmy67% (3)
- 2018 NCLEX-PN Test Prep. Questions and Answers with Explanations: Study Guide to Pass the License Exam Effortlessly - Exam Review for Practical NursesD'Everand2018 NCLEX-PN Test Prep. Questions and Answers with Explanations: Study Guide to Pass the License Exam Effortlessly - Exam Review for Practical NursesÉvaluation : 4.5 sur 5 étoiles4.5/5 (2)
- Exam Facts NCLEX PN Nursing Study GuideD'EverandExam Facts NCLEX PN Nursing Study GuideÉvaluation : 3.5 sur 5 étoiles3.5/5 (6)
- 2020 NCLEX-PN Test Prep. Questions and Answers with Explanations: Study Guide to Pass the License Exam Effortlessly - Exam Review for Practical NursesD'Everand2020 NCLEX-PN Test Prep. Questions and Answers with Explanations: Study Guide to Pass the License Exam Effortlessly - Exam Review for Practical NursesÉvaluation : 1 sur 5 étoiles1/5 (1)
- Nurses' Notes Date Shift Time Focus D-Data A-Action R-D - Patient WasDocument2 pagesNurses' Notes Date Shift Time Focus D-Data A-Action R-D - Patient WasMa Dionela EncinasPas encore d'évaluation
- Easy Nursing Notes For The Registered Nurse.D'EverandEasy Nursing Notes For The Registered Nurse.Évaluation : 4 sur 5 étoiles4/5 (6)
- Nursing Note Sample 17Document6 pagesNursing Note Sample 17Lanzen Dragneel100% (1)
- Sample Nurses Notes CuDocument3 pagesSample Nurses Notes Cuapi-1978086589% (19)
- 2017 NCLEX-RN Test Prep Questions and Answers with Explanations: Study Guide to Pass the License Exam EffortlesslyD'Everand2017 NCLEX-RN Test Prep Questions and Answers with Explanations: Study Guide to Pass the License Exam EffortlesslyÉvaluation : 4 sur 5 étoiles4/5 (18)
- Narrative ChartingDocument2 pagesNarrative Chartingearl_llamas0% (2)
- Chicago Review Press NCLEX-PN Practice Test and ReviewD'EverandChicago Review Press NCLEX-PN Practice Test and ReviewÉvaluation : 4 sur 5 étoiles4/5 (4)
- Nursing Note Sample 0009Document6 pagesNursing Note Sample 0009Lanzen DragneelPas encore d'évaluation
- Nurses Notes1Document1 pageNurses Notes1Wally Cuaresma67% (3)
- Sample Charting Trach CareDocument1 pageSample Charting Trach Caredoirge47100% (8)
- Nurses NotesDocument37 pagesNurses NotesTanya Book Hughes97% (30)
- Narrative ChartDocument5 pagesNarrative Charthady920100% (1)
- San Pedro Hospital of Davao City, Inc.: Nurses' NotesDocument3 pagesSan Pedro Hospital of Davao City, Inc.: Nurses' NotesJhulia GamutinPas encore d'évaluation
- Nursery ChartingDocument3 pagesNursery ChartingRI NAPas encore d'évaluation
- Focus Charting Example PDFDocument1 pageFocus Charting Example PDFRegine Lorenzana Mey-AngPas encore d'évaluation
- Nurses Notes SampleDocument3 pagesNurses Notes SampleleoPas encore d'évaluation
- Nursing Notes SampleDocument1 pageNursing Notes Samplelhdepuy100% (8)
- Nurse'S Notes: Bautista A 58 2021-0000025 Milagros F Medical Ward-207Document5 pagesNurse'S Notes: Bautista A 58 2021-0000025 Milagros F Medical Ward-207Renea Joy ArruejoPas encore d'évaluation
- DAR ChartingDocument2 pagesDAR ChartingJed Visaya83% (6)
- Delivery Nurses NotesDocument2 pagesDelivery Nurses NotesRS Buenavista67% (3)
- San Pedro Hospital of Davao City, Inc.: Nurses' NotesDocument2 pagesSan Pedro Hospital of Davao City, Inc.: Nurses' NotesSophia Jay LauriePas encore d'évaluation
- Documentation in NursingDocument43 pagesDocumentation in NursingMAHMOOD AHMED100% (19)
- Sample Dar ChartingDocument3 pagesSample Dar ChartingAl Lakah75% (4)
- ChartingDocument1 pageChartingberhanubedassa100% (2)
- Form 10 Nurse's NotesDocument5 pagesForm 10 Nurse's NotesJanelle Cabida SupnadPas encore d'évaluation
- Head To Toe Narrative ChartingDocument1 pageHead To Toe Narrative ChartingDianne Macaraig100% (3)
- LIM NursesNotesDocument2 pagesLIM NursesNotesSophia limPas encore d'évaluation
- Nurses NotesDocument2 pagesNurses NotesAvyel Kram100% (3)
- Nueva Ecija University of Science and TechnologyDocument3 pagesNueva Ecija University of Science and TechnologyRay Anne GonzalesPas encore d'évaluation
- Head To Toe Assessment in 5 Minutes or MoreDocument12 pagesHead To Toe Assessment in 5 Minutes or MoreTSPANPas encore d'évaluation
- Focus ChartingDocument6 pagesFocus ChartingChie Suarez100% (3)
- SampleCharting 418Document2 pagesSampleCharting 418Lai KuanlinPas encore d'évaluation
- Focus Charting of FDocument12 pagesFocus Charting of FRobert Rivas0% (2)
- 05 Nursing Note SampleDocument3 pages05 Nursing Note Sampletesttest testPas encore d'évaluation
- Day 1 Nurses NotesDocument13 pagesDay 1 Nurses Notesapi-265625311100% (1)
- Charting Basics: What Is Documentation?Document11 pagesCharting Basics: What Is Documentation?farahdlc100% (1)
- Nurses Notes 11Document1 pageNurses Notes 11janna mae patriarcaPas encore d'évaluation
- Nurses Progress Notes Name of Patient Attending Physician Room/Ward Hospital NoDocument1 pageNurses Progress Notes Name of Patient Attending Physician Room/Ward Hospital NoMr rawrPas encore d'évaluation
- Focus Data ChartingDocument3 pagesFocus Data ChartingcattleyaPas encore d'évaluation
- Nurses Notes TBDocument4 pagesNurses Notes TBSanvar Mal Soni0% (2)
- Sample Fous Charting Templates: Nurses' Progress Notes AdmissionDocument10 pagesSample Fous Charting Templates: Nurses' Progress Notes AdmissionLevy Garcia Sanchez100% (1)
- Nle Dec 07 Np1 RatioDocument23 pagesNle Dec 07 Np1 RatioJerwin CapurasPas encore d'évaluation
- Pain Care PlanDocument18 pagesPain Care Planjordanw0613Pas encore d'évaluation
- Patient Name: Lorna Dimagiba Age: 84 Years Old Gender: Female C.S: Widow BED#: #1Document3 pagesPatient Name: Lorna Dimagiba Age: 84 Years Old Gender: Female C.S: Widow BED#: #1Girlie MebañaPas encore d'évaluation
- Case Study - CvaDocument3 pagesCase Study - CvaJrBong Semanero50% (2)
- Physical Assessment CheatDocument7 pagesPhysical Assessment CheatJepe Urate100% (1)
- Nursing Notes Templates (Guidelines To Take Nursing Notes)Document20 pagesNursing Notes Templates (Guidelines To Take Nursing Notes)Rose100% (1)
- Focus Charting (DAR)Document1 pageFocus Charting (DAR)Raisa Robelle QuichoPas encore d'évaluation
- GROUP 6 ASSIGNMENT 1 Edited 4 Nov 09Document6 pagesGROUP 6 ASSIGNMENT 1 Edited 4 Nov 09Aaron WallacePas encore d'évaluation
- Renr Practice Test 11Document17 pagesRenr Practice Test 11Aaron Wallace92% (12)
- Nursing Council CXC Past Paper MCQ (1) (319) IMPORTANTDocument25 pagesNursing Council CXC Past Paper MCQ (1) (319) IMPORTANTAaron Wallace88% (32)
- Nurs Council TopicsDocument1 pageNurs Council TopicsAaron Wallace100% (1)
- Apirl 2001 Paper 2 (CL)Document15 pagesApirl 2001 Paper 2 (CL)Aaron Wallace100% (1)
- Chapter 1 Intro To Medical AssistingDocument16 pagesChapter 1 Intro To Medical AssistingAaron WallacePas encore d'évaluation
- Fire ExtinguisherDocument21 pagesFire Extinguisheramit dhingraPas encore d'évaluation
- Beka LambDocument41 pagesBeka LambKia-Marie ParsonsPas encore d'évaluation
- Vascular Disorder Case StudyDocument3 pagesVascular Disorder Case StudyAaron Wallace100% (1)
- Case Study Answers (Respiratory System)Document2 pagesCase Study Answers (Respiratory System)Aaron WallacePas encore d'évaluation
- Psychology TheoriesDocument7 pagesPsychology TheoriesAaron WallacePas encore d'évaluation
- What Is AdpieDocument5 pagesWhat Is AdpieAaron WallacePas encore d'évaluation
- Asthma MedicationsDocument3 pagesAsthma MedicationsAaron WallacePas encore d'évaluation
- A Kestrel For A Knave - WikipediaDocument26 pagesA Kestrel For A Knave - WikipediaAaron WallacePas encore d'évaluation
- 21stCenturyBusiness Curry Peck TheFuturesCompany2014Document45 pages21stCenturyBusiness Curry Peck TheFuturesCompany2014ericroyalPas encore d'évaluation
- Acute Renal Failure ManagementDocument15 pagesAcute Renal Failure ManagementAaron WallacePas encore d'évaluation
- Academic Year 2017-2018 - Short Course Advertisement Semester IIDocument17 pagesAcademic Year 2017-2018 - Short Course Advertisement Semester IINikita JacobsPas encore d'évaluation
- 1503 KJSDLJFLSDF X10Document219 pages1503 KJSDLJFLSDF X10Aaron WallacePas encore d'évaluation
- SEPT 9 2016 CPE Short-Courses1Document1 pageSEPT 9 2016 CPE Short-Courses1Aaron WallacePas encore d'évaluation
- Phelebotomy Answers 01 2018Document61 pagesPhelebotomy Answers 01 2018Aaron Wallace100% (1)
- Chapter 6Document15 pagesChapter 6Aaron WallacePas encore d'évaluation
- Angina ManagementDocument14 pagesAngina ManagementAaron WallacePas encore d'évaluation
- BSN 2 Specialties May-Aug 2014Document28 pagesBSN 2 Specialties May-Aug 2014Aaron WallacePas encore d'évaluation
- Consulting-Ten Commandments of Small Business (Lesson)Document1 pageConsulting-Ten Commandments of Small Business (Lesson)nenu_100Pas encore d'évaluation
- Scan0010 RotatedDocument12 pagesScan0010 RotatedAaron Wallace100% (3)
- Pathohys II-respiratory DiseasesDocument89 pagesPathohys II-respiratory DiseasesAaron WallacePas encore d'évaluation
- Cardiac System MedicationsDocument4 pagesCardiac System MedicationsfranjoyPas encore d'évaluation
- Asthma MedicationsDocument3 pagesAsthma MedicationsAaron WallacePas encore d'évaluation
- International Women Day 2017Document1 pageInternational Women Day 2017Aaron WallacePas encore d'évaluation
- Renr Review Program 2016Document8 pagesRenr Review Program 2016Aaron Wallace100% (2)
- RMC No. 23-2007-Government Payments WithholdingDocument7 pagesRMC No. 23-2007-Government Payments WithholdingWizardche_13Pas encore d'évaluation
- Spaces For Conflict and ControversiesDocument5 pagesSpaces For Conflict and ControversiesVistalPas encore d'évaluation
- Quanser Active Mass Damper UserManual PDFDocument21 pagesQuanser Active Mass Damper UserManual PDFCHAVEZ MURGA ARTURO ALEJANDROPas encore d'évaluation
- High-Performance Cutting and Grinding Technology For CFRP (Carbon Fiber Reinforced Plastic)Document7 pagesHigh-Performance Cutting and Grinding Technology For CFRP (Carbon Fiber Reinforced Plastic)Dongxi LvPas encore d'évaluation
- Text Mohamed AliDocument2 pagesText Mohamed AliARYAJAI SINGHPas encore d'évaluation
- Network Monitoring & Forensics: Jim IrvingDocument102 pagesNetwork Monitoring & Forensics: Jim IrvingKarel GoldmannPas encore d'évaluation
- Unibertsitaterako Hautaproba Ingelesa EHU/UPVDocument2 pagesUnibertsitaterako Hautaproba Ingelesa EHU/UPVdabidPas encore d'évaluation
- 3RD Last RPHDocument5 pages3RD Last RPHAdil Mohamad KadriPas encore d'évaluation
- Mudbound: Virgil Williams and Dee ReesDocument125 pagesMudbound: Virgil Williams and Dee Reesmohan kumarPas encore d'évaluation
- Wa0006.Document8 pagesWa0006.Poonm ChoudharyPas encore d'évaluation
- Fort St. John 108 Street & Alaska Highway IntersectionDocument86 pagesFort St. John 108 Street & Alaska Highway IntersectionAlaskaHighwayNewsPas encore d'évaluation
- Women in IslamDocument22 pagesWomen in Islamsayed Tamir janPas encore d'évaluation
- WWW - Nswkendo IaidoDocument1 pageWWW - Nswkendo IaidoAshley AndersonPas encore d'évaluation
- Minimalist Aesthetics Business Plan by SlidesgoDocument63 pagesMinimalist Aesthetics Business Plan by Slidesgorandom potatoPas encore d'évaluation
- Lae 3333 2 Week Lesson PlanDocument37 pagesLae 3333 2 Week Lesson Planapi-242598382Pas encore d'évaluation
- Using JAXB For XML With Java - DZone JavaDocument20 pagesUsing JAXB For XML With Java - DZone JavajaehooPas encore d'évaluation
- PMP Chapter-12 P. Procurement ManagementDocument30 pagesPMP Chapter-12 P. Procurement Managementashkar299Pas encore d'évaluation
- Algebra Lineal Septima Edicion Stanley I. Grossman S. Mcgraw-Hilliinteramericana Editores S.A. de C.V Mexico, DFDocument1 pageAlgebra Lineal Septima Edicion Stanley I. Grossman S. Mcgraw-Hilliinteramericana Editores S.A. de C.V Mexico, DFJOSE JULIAN RAMIREZ ROJASPas encore d'évaluation
- Media Planning Is Generally The Task of A Media Agency and Entails Finding The Most Appropriate Media Platforms For A ClientDocument11 pagesMedia Planning Is Generally The Task of A Media Agency and Entails Finding The Most Appropriate Media Platforms For A ClientDaxesh Kumar BarotPas encore d'évaluation
- 173544avaya Aura AES 7-0 JTAPI Programmers GuideDocument88 pages173544avaya Aura AES 7-0 JTAPI Programmers GuideAhmed SakrPas encore d'évaluation
- Sap Successfactors Training Materials Guide: April 2020Document4 pagesSap Successfactors Training Materials Guide: April 2020pablo picassoPas encore d'évaluation
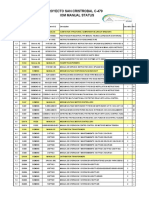
- Proyecto San Cristrobal C-479 Iom Manual StatusDocument18 pagesProyecto San Cristrobal C-479 Iom Manual StatusAllen Marcelo Ballesteros LópezPas encore d'évaluation
- The Relationship Between Law and MoralityDocument12 pagesThe Relationship Between Law and MoralityAnthony JosephPas encore d'évaluation
- History of Architecture VI: Unit 1Document20 pagesHistory of Architecture VI: Unit 1Srehari100% (1)
- 215 Final Exam Formula SheetDocument2 pages215 Final Exam Formula SheetH.C. Z.Pas encore d'évaluation
- Lozada Vs MendozaDocument4 pagesLozada Vs MendozaHarold EstacioPas encore d'évaluation
- Court Documents From Toronto Police Project Brazen - Investigation of Alexander "Sandro" Lisi and Toronto Mayor Rob FordDocument474 pagesCourt Documents From Toronto Police Project Brazen - Investigation of Alexander "Sandro" Lisi and Toronto Mayor Rob Fordanna_mehler_papernyPas encore d'évaluation
- The Confederation or Fraternity of Initiates (1941)Document82 pagesThe Confederation or Fraternity of Initiates (1941)Clymer777100% (1)
- FCI - GST - Manual On Returns and PaymentsDocument30 pagesFCI - GST - Manual On Returns and PaymentsAmber ChaturvediPas encore d'évaluation
- United States Court of Appeals Fifth CircuitDocument4 pagesUnited States Court of Appeals Fifth CircuitScribd Government DocsPas encore d'évaluation