Vous aimerez peut-être aussi
- Algo Pals TachycardiaDocument1 pageAlgo Pals TachycardiaArdie FratamaPas encore d'évaluation
- Pediatric Tachycardia With A Pulse Algorithm: Yes NoDocument1 pagePediatric Tachycardia With A Pulse Algorithm: Yes NoRatna TambaPas encore d'évaluation
- With A Pulse and Poor Perfusion: Pediatric TachycardiaDocument1 pageWith A Pulse and Poor Perfusion: Pediatric TachycardiaIin-Ignasia Diahayujulindah Mujiman0% (1)
- Managemen Disritmia: Dr. Rofika Hanifa, SPPDDocument20 pagesManagemen Disritmia: Dr. Rofika Hanifa, SPPDavivlabirdPas encore d'évaluation
- Onlinemeded Notes CardioDocument1 pageOnlinemeded Notes CardioCourtney HolbrookPas encore d'évaluation
- Advanced Cardiac Life SupportDocument37 pagesAdvanced Cardiac Life SupportRoy Acosta GumbanPas encore d'évaluation
- G2015 Adult Tachycardia PDFDocument1 pageG2015 Adult Tachycardia PDFPlabber JunePas encore d'évaluation
- G2015 Adult Tachycardia PDFDocument1 pageG2015 Adult Tachycardia PDFibbs91Pas encore d'évaluation
- 26) Approach To Pediatric ArrhythmiasDocument44 pages26) Approach To Pediatric ArrhythmiasJude AlyousefPas encore d'évaluation
- Tachycardia AlgorythmDocument1 pageTachycardia AlgorythmUZNAPMPas encore d'évaluation
- ACLS AritmiaDocument18 pagesACLS AritmiaZega AgustianPas encore d'évaluation
- Pediatric Bradycardia With A Pulse and Poor Perfusion AlgorithmDocument1 pagePediatric Bradycardia With A Pulse and Poor Perfusion AlgorithmRadhiatul MardhiahPas encore d'évaluation
- Adult Tachycardia (With Pulse) AlgorithmDocument1 pageAdult Tachycardia (With Pulse) AlgorithmJames ChoiPas encore d'évaluation
- Tachycardia AlgorithmDocument1 pageTachycardia AlgorithmGideon BahulePas encore d'évaluation
- .JPG 958×1,280 PixelsDocument1 page.JPG 958×1,280 Pixelsyordanos getachewPas encore d'évaluation
- 5.ALS Algorithms TachycardiaDocument1 page5.ALS Algorithms TachycardiaMassimo Di BenedettoPas encore d'évaluation
- Bradycardia and TachycardiaDocument66 pagesBradycardia and TachycardiaKarissaPas encore d'évaluation
- Rate P Wave QRS Comple X PR Interval: ST RDDocument2 pagesRate P Wave QRS Comple X PR Interval: ST RDPat G.Pas encore d'évaluation
- Pals Pediatric BradycardiaDocument1 pagePals Pediatric BradycardiadarlingcarvajalduquePas encore d'évaluation
- Assess Appropriateness For Clinical Condition. Heart Rate Typically 150/min If TachyarrhythmiaDocument1 pageAssess Appropriateness For Clinical Condition. Heart Rate Typically 150/min If TachyarrhythmiaSiti Nur R Firda FauziyahPas encore d'évaluation
- AdultTachycardiaWithPulse AlgorithmDocument1 pageAdultTachycardiaWithPulse AlgorithmIsmail SlimPas encore d'évaluation
- ALS Algorithms LS Tachycardia 2.0Document1 pageALS Algorithms LS Tachycardia 2.0Lucian Alin DinuPas encore d'évaluation
- Algo Tachycardia PDFDocument1 pageAlgo Tachycardia PDFYudhistira AdiPas encore d'évaluation
- Simplified ACLS AlgorithmDocument1 pageSimplified ACLS AlgorithmBrianPas encore d'évaluation
- ACLS Tachycardia Algorithm For Managing Stable TachycardiaDocument4 pagesACLS Tachycardia Algorithm For Managing Stable TachycardiaLady MuffinsPas encore d'évaluation
- ACLS AritmiaDocument18 pagesACLS AritmiaZega AgustianPas encore d'évaluation
- Ecg ReadingsDocument11 pagesEcg ReadingsAnton Laurenciana100% (5)
- Tachycardia With A Pulse Algorithm: Assess Appropriateness For Clinical ConditionDocument1 pageTachycardia With A Pulse Algorithm: Assess Appropriateness For Clinical ConditionDendy Frannuzul RamadhanPas encore d'évaluation
- AlgorithmACLStachycardiawithapulse PDFDocument1 pageAlgorithmACLStachycardiawithapulse PDFDendy Frannuzul RamadhanPas encore d'évaluation
- Tachycardia Algorithm 2021Document1 pageTachycardia Algorithm 2021Ravin DebiePas encore d'évaluation
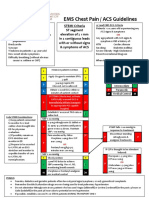
- EMS Chest Pain / ACS GuidelinesDocument1 pageEMS Chest Pain / ACS GuidelinesJuanaly BadiolaPas encore d'évaluation
- NCM 112 MSN Prelim Topic 4 Cardiac Rhythm DisordersDocument5 pagesNCM 112 MSN Prelim Topic 4 Cardiac Rhythm DisordersKim Erida QuezonPas encore d'évaluation
- Nursing CS Treatment-Of-Atrial-Dysrhythmias 02Document1 pageNursing CS Treatment-Of-Atrial-Dysrhythmias 02frankshro156Pas encore d'évaluation
- Antiarrythmic Agents: Antiarrythmic Drugs For HorsesDocument3 pagesAntiarrythmic Agents: Antiarrythmic Drugs For HorsesMageja TatendaPas encore d'évaluation
- Algo Bradycardia DikonversiDocument5 pagesAlgo Bradycardia DikonversiDaniel SitungkirPas encore d'évaluation
- EKG Nclex High YieldDocument13 pagesEKG Nclex High Yieldnene lewis100% (1)
- Shock: Shout For Help/Activate Emergency ResponseDocument6 pagesShock: Shout For Help/Activate Emergency ResponseandiyanimalikPas encore d'évaluation
- High Yield Surgery Compatible Version PDFDocument20 pagesHigh Yield Surgery Compatible Version PDFSurgery CSC1Pas encore d'évaluation
- DKA Protocol With Calculation SheetDocument7 pagesDKA Protocol With Calculation SheetAmanda Marie Best OsbournePas encore d'évaluation
- Ecg Dysrythmias Nursing Responsibilitu Sinus Node 1.) Sinus BradycardiaDocument2 pagesEcg Dysrythmias Nursing Responsibilitu Sinus Node 1.) Sinus BradycardiaNickha LazoPas encore d'évaluation
- Neonate / Infant Child / AdultDocument1 pageNeonate / Infant Child / AdultRizky Ayu RPas encore d'évaluation
- ACLS Cardiac Arrest Algorithm For Suspected or Confirmed COVID-19 PatientsDocument2 pagesACLS Cardiac Arrest Algorithm For Suspected or Confirmed COVID-19 PatientsDeny PamungkasPas encore d'évaluation
- ACLS 2020 Algorithms: American Heart Association 2020 GuidelinesDocument8 pagesACLS 2020 Algorithms: American Heart Association 2020 GuidelinesNofi Nurina100% (4)
- Screenshot 2565-05-03 at 10.34.19Document39 pagesScreenshot 2565-05-03 at 10.34.19Sugus PichayaPas encore d'évaluation
- Anesthesia Pocket Guide 2020 PDFDocument2 pagesAnesthesia Pocket Guide 2020 PDFMaksym DemianchukPas encore d'évaluation
- Arrhythmias EmergencyDocument10 pagesArrhythmias EmergencyNITACORDEIROPas encore d'évaluation
- Algorithm Tatalaksana Kelainan KongenitalDocument32 pagesAlgorithm Tatalaksana Kelainan KongenitalLa Ode Muhammadin MatahanaPas encore d'évaluation
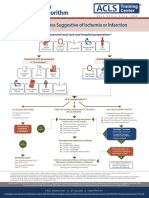
- Syndromes Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital PreparationDocument1 pageSyndromes Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital PreparationIGOR SHEYNINPas encore d'évaluation
- Algoritma Ambulance - PHCDocument11 pagesAlgoritma Ambulance - PHCYassarPas encore d'évaluation
- Algo Acs PDFDocument1 pageAlgo Acs PDFJim Christian EllaserPas encore d'évaluation
- Algo Acs PDFDocument1 pageAlgo Acs PDFNety Pandung SalembanPas encore d'évaluation
- Venticular DysrthytmiasDocument3 pagesVenticular DysrthytmiasKaye Marie OportoPas encore d'évaluation
- Acut Coronary SyndromesDocument1 pageAcut Coronary SyndromesMuhittin Selçuk ÖzkanPas encore d'évaluation
- Nihms 1646158Document30 pagesNihms 1646158darlingcarvajalduquePas encore d'évaluation
- Updated Nomenclature of DeliriumDocument3 pagesUpdated Nomenclature of Deliriumken barrios montalvoPas encore d'évaluation
- Pediatric Pain AssessmentDocument10 pagesPediatric Pain AssessmentdarlingcarvajalduquePas encore d'évaluation
- Misc AbdomenDocument8 pagesMisc AbdomendarlingcarvajalduquePas encore d'évaluation
- Stollings2021 Article DeliriumInCriticalIllnessCliniDocument15 pagesStollings2021 Article DeliriumInCriticalIllnessCliniJavier BlancPas encore d'évaluation
- Httpswatermark Silverchair Com - Ezproxy.unbosque - edu.Copedsinreview.2022005642.Pdftoken AQECAHi208BE49Ooan9kkhW Ercy7Dm3ZL 9Document10 pagesHttpswatermark Silverchair Com - Ezproxy.unbosque - edu.Copedsinreview.2022005642.Pdftoken AQECAHi208BE49Ooan9kkhW Ercy7Dm3ZL 9darlingcarvajalduquePas encore d'évaluation
- Prevención Neumonia Asociada A Ventilación.Document19 pagesPrevención Neumonia Asociada A Ventilación.darlingcarvajalduquePas encore d'évaluation
- PADIS Guidelines Teaching Slides ImmobilityDocument25 pagesPADIS Guidelines Teaching Slides ImmobilityDaniel Lago BorgesPas encore d'évaluation
- ESPNIC Guidance On The Management of The Deteriorating Child or Cardiac Arrest of Suspected or Proven COVID FINAL PDFDocument2 pagesESPNIC Guidance On The Management of The Deteriorating Child or Cardiac Arrest of Suspected or Proven COVID FINAL PDFdarlingcarvajalduquePas encore d'évaluation
- De-Escalation of Critical Care and Prevention of Iatrogenicity Through PICU Liberation Rounding Process and A Daily Rounding ChecklistDocument1 pageDe-Escalation of Critical Care and Prevention of Iatrogenicity Through PICU Liberation Rounding Process and A Daily Rounding ChecklistdarlingcarvajalduquePas encore d'évaluation
- Early Progressive Mobility Protocol: Step 1: Screen For SafetyDocument2 pagesEarly Progressive Mobility Protocol: Step 1: Screen For SafetydarlingcarvajalduquePas encore d'évaluation
- Post-Intensive Care Syndrome: Its Pathophysiology, Prevention, and Future DirectionsDocument14 pagesPost-Intensive Care Syndrome: Its Pathophysiology, Prevention, and Future DirectionsdarlingcarvajalduquePas encore d'évaluation
- Getattachmentnonopioid Medication Options PDFDocument1 pageGetattachmentnonopioid Medication Options PDFdarlingcarvajalduquePas encore d'évaluation
- Drug Doses 2017Document127 pagesDrug Doses 2017Yuliawati HarunaPas encore d'évaluation
- Torsade de Pointes - The Clinical Considerations PDFDocument6 pagesTorsade de Pointes - The Clinical Considerations PDFdarlingcarvajalduquePas encore d'évaluation
- Early Progressive Mobility Protocol: Step 1: Screen For SafetyDocument2 pagesEarly Progressive Mobility Protocol: Step 1: Screen For SafetydarlingcarvajalduquePas encore d'évaluation
- PALS Algorithms 2019 (Pediatric Advanced Life Support)Document1 pagePALS Algorithms 2019 (Pediatric Advanced Life Support)darlingcarvajalduquePas encore d'évaluation
- Avances en Ultrasonido Pediatria oDocument7 pagesAvances en Ultrasonido Pediatria odarlingcarvajalduquePas encore d'évaluation
- Q SofaDocument9 pagesQ SofadarlingcarvajalduquePas encore d'évaluation
- 2020 ESPNIC PEMVECC COVID-19 Practice RecommendationsDocument7 pages2020 ESPNIC PEMVECC COVID-19 Practice RecommendationsdmallozziPas encore d'évaluation
- Protocolo FATE (Eco TT)Document4 pagesProtocolo FATE (Eco TT)darlingcarvajalduquePas encore d'évaluation
- Mortalidad e Hipotermia Vs NormotermiaDocument8 pagesMortalidad e Hipotermia Vs NormotermiadarlingcarvajalduquePas encore d'évaluation
- Choque Cardiogenico MicrocirculacionDocument6 pagesChoque Cardiogenico MicrocirculaciondarlingcarvajalduquePas encore d'évaluation
- Q SofaDocument9 pagesQ SofadarlingcarvajalduquePas encore d'évaluation
- Pals 2015 Documento CompletoDocument50 pagesPals 2015 Documento CompletodarlingcarvajalduquePas encore d'évaluation
- 2015 AHA Guidelines Highlights EnglishDocument36 pages2015 AHA Guidelines Highlights EnglishshiloinPas encore d'évaluation
- Pals Pediatric BradycardiaDocument1 pagePals Pediatric BradycardiadarlingcarvajalduquePas encore d'évaluation
- Posición PronoDocument6 pagesPosición PronodarlingcarvajalduquePas encore d'évaluation
- ANTIARRITMICOSDocument9 pagesANTIARRITMICOSdarlingcarvajalduquePas encore d'évaluation
- G O Ms NoDocument2 pagesG O Ms NoMuralidhar MogalicherlaPas encore d'évaluation
- Safe Work Method Statement TemplateDocument5 pagesSafe Work Method Statement Templatebmb00Pas encore d'évaluation
- Flinn (ISA 315 + ISA 240 + ISA 570)Document2 pagesFlinn (ISA 315 + ISA 240 + ISA 570)Zareen AbbasPas encore d'évaluation
- 1 Why The Working Class?: Education For SocialistsDocument32 pages1 Why The Working Class?: Education For SocialistsDrew PoveyPas encore d'évaluation
- Financial Accounting Harrison 10th Edition Test BankDocument24 pagesFinancial Accounting Harrison 10th Edition Test BankNicoleHallrktc100% (46)
- The Defense of The Faith Cornelius Van TilDocument8 pagesThe Defense of The Faith Cornelius Van TilEmanuel Gutiérrez100% (1)
- Affidavit of FactDocument3 pagesAffidavit of FactMortgage Compliance Investigators100% (8)
- Investment Phase of Desire EngineDocument21 pagesInvestment Phase of Desire EngineNir Eyal100% (1)
- LIBOR Transition Bootcamp 2021Document11 pagesLIBOR Transition Bootcamp 2021Eliza MartinPas encore d'évaluation
- SSL-VPN Service: End User GuideDocument19 pagesSSL-VPN Service: End User Guideumer.shariff87Pas encore d'évaluation
- Rules and Regulations For Cottage Booking PDFDocument1 pageRules and Regulations For Cottage Booking PDFmrinmoy chakrabortyPas encore d'évaluation
- October Free Chapter - Deranged Marriage by Sushi DasDocument24 pagesOctober Free Chapter - Deranged Marriage by Sushi DasRandomHouseAUPas encore d'évaluation
- Cruttenden (2014) : (Summary)Document2 pagesCruttenden (2014) : (Summary)Emma PeelPas encore d'évaluation
- Emerging Trends in Recruitment and Talent AcquisitionDocument3 pagesEmerging Trends in Recruitment and Talent Acquisitionpallavi1289Pas encore d'évaluation
- Cheat Sheet - Logistics Term & Salary DetailsDocument4 pagesCheat Sheet - Logistics Term & Salary Detailstaseenzaheer33Pas encore d'évaluation
- Abm 12 Marketing q1 Clas2 Relationship Marketing v1 - Rhea Ann NavillaDocument13 pagesAbm 12 Marketing q1 Clas2 Relationship Marketing v1 - Rhea Ann NavillaKim Yessamin MadarcosPas encore d'évaluation
- Upstream Pre B1 Unit Test 9Document3 pagesUpstream Pre B1 Unit Test 9Biljana NestorovskaPas encore d'évaluation
- Chinese Dipping SauceDocument11 pagesChinese Dipping Sauceb.dutta100% (1)
- SP BVL Peru General Index ConstituentsDocument2 pagesSP BVL Peru General Index ConstituentsMiguelQuispeHuaringaPas encore d'évaluation
- Apology StrategiesDocument7 pagesApology StrategiesAdriana MancașPas encore d'évaluation
- Can Chatgpt Help Improve CybersecurityDocument2 pagesCan Chatgpt Help Improve CybersecurityVisiontech InternationalPas encore d'évaluation
- 2022 P6 Maths Prelim NanyangDocument52 pages2022 P6 Maths Prelim NanyangAlbert Hein Nyan HtetPas encore d'évaluation
- Malimono Campus Learning Continuity PlanDocument7 pagesMalimono Campus Learning Continuity PlanEmmylou BorjaPas encore d'évaluation
- Account StatementDocument12 pagesAccount StatementNarendra PPas encore d'évaluation
- Case Study On Federal ExpressDocument3 pagesCase Study On Federal ExpressDipanjan RoychoudharyPas encore d'évaluation
- Succession: ElementsDocument33 pagesSuccession: ElementsDave A ValcarcelPas encore d'évaluation
- Ch.3 Accounting of Employee Stock Option PlansDocument4 pagesCh.3 Accounting of Employee Stock Option PlansDeepthi R TejurPas encore d'évaluation
- Cost-Effective Sustainable Design & ConstructionDocument6 pagesCost-Effective Sustainable Design & ConstructionKeith Parker100% (2)
- Earning Updates (Company Update)Document93 pagesEarning Updates (Company Update)Shyam SunderPas encore d'évaluation
- Helena Monolouge From A Midsummer Night's DreamDocument2 pagesHelena Monolouge From A Midsummer Night's DreamKayla Grimm100% (1)