Vous aimerez peut-être aussi
- Complete Guide To Physical ExamDocument19 pagesComplete Guide To Physical ExamSeff Causapin100% (2)
- Systemic Lupus Erythematosus PathophysiologyDocument8 pagesSystemic Lupus Erythematosus Pathophysiologykathy92% (24)
- SLE ANEMIA PATHOPHYSIOLOGYDocument1 pageSLE ANEMIA PATHOPHYSIOLOGYGhan Maria100% (2)
- MEASLES PresentationDocument29 pagesMEASLES PresentationMobin Ur Rehman Khan100% (3)
- SLE Risk Factors and ComplicationsDocument5 pagesSLE Risk Factors and Complicationsjoyrena ochondraPas encore d'évaluation
- Pathophysiology - Rheumatoid ArthritisDocument1 pagePathophysiology - Rheumatoid ArthritisAngel FiloteoPas encore d'évaluation
- Pathophysiology of TuberculosisDocument2 pagesPathophysiology of TuberculosisLeikkaPas encore d'évaluation
- Fibroid & Cyst ProtocolDocument32 pagesFibroid & Cyst ProtocolTheresa DalePas encore d'évaluation
- Systemic Lupus Erythematosus PathophysiologyDocument8 pagesSystemic Lupus Erythematosus PathophysiologySharmaineTaguitagOmli100% (1)
- SLE Patogenesis & Patofisiologi PDFDocument8 pagesSLE Patogenesis & Patofisiologi PDFRIZQI IRFANSYAH100% (1)
- Sysemic Lupus Erythematosus Case StudyDocument53 pagesSysemic Lupus Erythematosus Case StudyJennylen Torres100% (1)
- Pathophysiology of Rheumatoid ArthritisDocument1 pagePathophysiology of Rheumatoid ArthritisGerardeanne ReposarPas encore d'évaluation
- Systemic Lupus ErythematosusDocument80 pagesSystemic Lupus ErythematosusLarissa Miguel Severa100% (2)
- Systemic Lupus ErythematosusDocument31 pagesSystemic Lupus ErythematosusJerilee SoCute WattsPas encore d'évaluation
- Physical Diagnosis of The ThoraxDocument3 pagesPhysical Diagnosis of The ThoraxSeff Causapin100% (1)
- A Case Study On Systemic Lupus ErythematosusDocument19 pagesA Case Study On Systemic Lupus ErythematosusIrah GatchoPas encore d'évaluation
- Pa Tho Physiology Sle, CompDocument5 pagesPa Tho Physiology Sle, CompHassan Bj MarabongPas encore d'évaluation
- Anemia PathophysiologyDocument2 pagesAnemia PathophysiologyHoney Lorie D. Simbajon67% (6)
- Patho of Pott's DiseaseDocument2 pagesPatho of Pott's DiseaseIris Balino100% (1)
- Laboratory and Diagnostic Findings: Small Cell CarcinomaDocument4 pagesLaboratory and Diagnostic Findings: Small Cell CarcinomaTheresa Sombilla FacunlaPas encore d'évaluation
- Biohackers Handbook ImmunityDocument37 pagesBiohackers Handbook ImmunityDaniel PopPas encore d'évaluation
- Salivary GlandsDocument68 pagesSalivary GlandsTatiana Decuseară100% (1)
- Harrison SLEDocument11 pagesHarrison SLEpazucenaPas encore d'évaluation
- A Case Study Presentation On Systemic Lupus Erythematosus - Group 1Document34 pagesA Case Study Presentation On Systemic Lupus Erythematosus - Group 1KeepItSecret100% (2)
- Chron's Disease 2Document3 pagesChron's Disease 2TarantadoPas encore d'évaluation
- Abdomen Physical DiagnosisDocument3 pagesAbdomen Physical DiagnosisSeff CausapinPas encore d'évaluation
- Systemic Lupus ErythematosusDocument4 pagesSystemic Lupus ErythematosusLau Colastre100% (1)
- Colloid Nodular GoiterDocument37 pagesColloid Nodular GoiterLori GeorgePas encore d'évaluation
- Sanitary Engineering2 (Repaired)Document95 pagesSanitary Engineering2 (Repaired)ronnel mauzar100% (2)
- SLE PathophysiologyDocument3 pagesSLE PathophysiologyRanela Kwinkee Pastor Salazar100% (7)
- Aseptic TechniqueDocument34 pagesAseptic TechniqueJessa Adenig100% (1)
- Sle FinalDocument41 pagesSle FinalAsniah Hadjiadatu Abdullah100% (1)
- Systemic Lupus Erythematosus (SLE) Is A Multiorgan System Autoimmune DiseaseDocument9 pagesSystemic Lupus Erythematosus (SLE) Is A Multiorgan System Autoimmune Diseasecoyre100% (2)
- Genital Tract Infections - GynecologyDocument17 pagesGenital Tract Infections - GynecologyKC Dela RosaPas encore d'évaluation
- Anterior Pituitary Tumor SyndromesDocument10 pagesAnterior Pituitary Tumor SyndromesSeff CausapinPas encore d'évaluation
- Anterior Pituitary Tumor SyndromesDocument10 pagesAnterior Pituitary Tumor SyndromesSeff CausapinPas encore d'évaluation
- Wilm's Tumor PathophysiologyDocument2 pagesWilm's Tumor PathophysiologyJonalene Suarez100% (2)
- LupusDocument28 pagesLupusRiin IrasustaPas encore d'évaluation
- SARS PowerpointDocument44 pagesSARS PowerpointXinn Xinn Vanzandt100% (1)
- Approach To Patient With Endocrine DisordersDocument2 pagesApproach To Patient With Endocrine DisordersSeff CausapinPas encore d'évaluation
- Musculoskeletal System Physical DiagnosisDocument4 pagesMusculoskeletal System Physical DiagnosisSeff Causapin100% (1)
- Sympathomimetic Agents: CLIN. PHARM (Dr. Salvador) Asthma 05 SEPT 2017Document3 pagesSympathomimetic Agents: CLIN. PHARM (Dr. Salvador) Asthma 05 SEPT 2017Seff Causapin100% (1)
- Bacterial and Viral MeningitisDocument12 pagesBacterial and Viral Meningitisapi-3704562Pas encore d'évaluation
- Physical Diagnosis of Cardiovascular SystemDocument6 pagesPhysical Diagnosis of Cardiovascular SystemSeff Causapin100% (1)
- Pathophysiology of TB MeningitisDocument1 pagePathophysiology of TB Meningitisreanzz100% (1)
- Pathophysiology of Multiple MyelomaDocument3 pagesPathophysiology of Multiple MyelomaRifa'atul Mahmudah100% (1)
- Myesthenia GravisDocument3 pagesMyesthenia GravisJorie RocoPas encore d'évaluation
- Pa Tho Physiology of Hodgkin'sDocument10 pagesPa Tho Physiology of Hodgkin'sIvica Rae100% (1)
- Systemic Lupus ErythematosusDocument2 pagesSystemic Lupus ErythematosusErnest canetePas encore d'évaluation
- Sericulture ManualDocument37 pagesSericulture ManualBabu Ram Panthi100% (10)
- PathoConceptMap AIDSDocument3 pagesPathoConceptMap AIDSKristen Babauta50% (2)
- Peripheral Vascular System Physical DiagnosisDocument3 pagesPeripheral Vascular System Physical DiagnosisSeff Causapin100% (1)
- Case of Febrile SeizuresDocument2 pagesCase of Febrile SeizuresAzizan HannyPas encore d'évaluation
- Infectious Mononucleosis Concept MapDocument4 pagesInfectious Mononucleosis Concept MapElle100% (1)
- Systemic Lupus Erythematosus PathophysiologyDocument8 pagesSystemic Lupus Erythematosus PathophysiologyAnonymous OU6w8lX9Pas encore d'évaluation
- SLE PathophysiologyDocument3 pagesSLE PathophysiologyyasiraPas encore d'évaluation
- Systemic Lupus ErythematosusDocument14 pagesSystemic Lupus ErythematosusArun ArachelvanPas encore d'évaluation
- Med 1.11 - SleDocument5 pagesMed 1.11 - SleZazaPas encore d'évaluation
- Pa Tho Physiology Part 1Document1 pagePa Tho Physiology Part 1anonymous89ify100% (2)
- Acute Lymphoblastic Leukemia Pathophysiology DiagramDocument3 pagesAcute Lymphoblastic Leukemia Pathophysiology DiagramChris FacundoPas encore d'évaluation
- Systemic Lupous Erythematosus (SLE)Document46 pagesSystemic Lupous Erythematosus (SLE)Power La Victoria Floro100% (1)
- Dengue PathophysiologyDocument1 pageDengue PathophysiologyRafael Miguel Alon Protacio50% (2)
- Lupus, SLEDocument2 pagesLupus, SLEFrances Anne Pasiliao100% (2)
- Rheumatoid ArthritisDocument25 pagesRheumatoid ArthritisGandung PrakosoPas encore d'évaluation
- DB13 - Pathophysiology of AtherosclerosisDocument2 pagesDB13 - Pathophysiology of Atherosclerosisi_vhie03Pas encore d'évaluation
- Precipitating Environmental Factors and Pathophysiology of Dengue VirusDocument4 pagesPrecipitating Environmental Factors and Pathophysiology of Dengue VirusKathleen DimacaliPas encore d'évaluation
- Pathophysiology of Burn Injury (1) DVDocument2 pagesPathophysiology of Burn Injury (1) DVRizzie Montes0% (1)
- Pott's DiseaseDocument8 pagesPott's DiseaseLorebell100% (2)
- Vii. Pathophysiology A. AlgorithmDocument2 pagesVii. Pathophysiology A. AlgorithmJonna Mae TurquezaPas encore d'évaluation
- Wilm's Tumor Pa Tho PhysiologyDocument1 pageWilm's Tumor Pa Tho Physiologya_yeLPas encore d'évaluation
- Case Study Acute Lymphoid LeukemiaDocument1 pageCase Study Acute Lymphoid Leukemia2literPas encore d'évaluation
- Factors and Symptoms of Bone CancerDocument3 pagesFactors and Symptoms of Bone CancerJenievieve MerzaPas encore d'évaluation
- Hepatoblastoma PathophysiologyDocument2 pagesHepatoblastoma Pathophysiologyjennachristy03100% (1)
- Pathophysiology of Alzheimers DiseaseDocument2 pagesPathophysiology of Alzheimers DiseaseJaysellePuguonTabijePas encore d'évaluation
- Pathophysiology of Nephrotic SyndromeDocument1 pagePathophysiology of Nephrotic SyndromeRan MaPas encore d'évaluation
- Case Study On LeukemiaDocument33 pagesCase Study On LeukemiaBhupesh PatidarPas encore d'évaluation
- Systemic Lupus Erythematosus (SLE) Pathogenesis and ManifestationsDocument10 pagesSystemic Lupus Erythematosus (SLE) Pathogenesis and Manifestationsinah krizia laguePas encore d'évaluation
- LP SLE Maulani Hendriyani RevisiDocument49 pagesLP SLE Maulani Hendriyani Revisimaulani hendriyani100% (1)
- Systemic Lupus Erythematosus: Pardis Nematollahi MD, ACP June, 2014Document50 pagesSystemic Lupus Erythematosus: Pardis Nematollahi MD, ACP June, 2014devPas encore d'évaluation
- Disorders of The Female Reproductive System PDFDocument4 pagesDisorders of The Female Reproductive System PDFSeff CausapinPas encore d'évaluation
- Dem Tickler NotesDocument1 pageDem Tickler NotesSeff CausapinPas encore d'évaluation
- 3 180824051636Document45 pages3 180824051636Seff CausapinPas encore d'évaluation
- Understanding Multinodular Non-Toxic GoiterDocument58 pagesUnderstanding Multinodular Non-Toxic GoiterSeff CausapinPas encore d'évaluation
- Hemostasissurgicalbleedingandtransfusion 130707035616 Phpapp02Document42 pagesHemostasissurgicalbleedingandtransfusion 130707035616 Phpapp02Seff CausapinPas encore d'évaluation
- Lumbar TapDocument4 pagesLumbar TapSeff CausapinPas encore d'évaluation
- Disorders of The Female Reproductive System PDFDocument4 pagesDisorders of The Female Reproductive System PDFSeff CausapinPas encore d'évaluation
- Altitude IllnessDocument4 pagesAltitude IllnessSeff CausapinPas encore d'évaluation
- Glomerular Diseases: Pathogenesis of Glomerular Diseases Progression of Glomerular DiseasesDocument6 pagesGlomerular Diseases: Pathogenesis of Glomerular Diseases Progression of Glomerular DiseasesSeff CausapinPas encore d'évaluation
- Urinary Tract Obstruction (UTO): Causes, Symptoms and DiagnosisDocument2 pagesUrinary Tract Obstruction (UTO): Causes, Symptoms and DiagnosisSeff CausapinPas encore d'évaluation
- Disorders of The MediastinumDocument1 pageDisorders of The MediastinumSeff CausapinPas encore d'évaluation
- Medicine (Dr. Pedroza) Copd 14 FEBRUARY 2018Document3 pagesMedicine (Dr. Pedroza) Copd 14 FEBRUARY 2018Seff CausapinPas encore d'évaluation
- Approach To The PX With CancerDocument7 pagesApproach To The PX With CancerSeff CausapinPas encore d'évaluation
- Tubulointerstitial DsesDocument3 pagesTubulointerstitial DsesSeff CausapinPas encore d'évaluation
- Disturbances in Respiratory FunctionDocument6 pagesDisturbances in Respiratory FunctionSeff CausapinPas encore d'évaluation
- MNGT of AmoebiasisDocument6 pagesMNGT of AmoebiasisSeff CausapinPas encore d'évaluation
- Clinicopathologic Narrative ReportDocument3 pagesClinicopathologic Narrative ReportSeff CausapinPas encore d'évaluation
- Salmon Ellos IsDocument3 pagesSalmon Ellos IsSeff CausapinPas encore d'évaluation
- LeptospirosisDocument2 pagesLeptospirosisSeff CausapinPas encore d'évaluation
- Leg Weakness PDFDocument8 pagesLeg Weakness PDFamamùra maamarPas encore d'évaluation
- AIDS and PeriodontiumDocument25 pagesAIDS and PeriodontiumKarthik Krishna M100% (1)
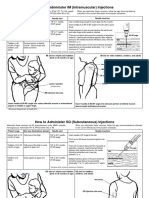
- Im SQ Admin PDFDocument2 pagesIm SQ Admin PDFAlvin JjPas encore d'évaluation
- MLS 223 Clinical Bacteriology Module 6 Unit 2Document28 pagesMLS 223 Clinical Bacteriology Module 6 Unit 2p7pxrdjhwvPas encore d'évaluation
- Adult HIV Notes On GuidelinesDocument423 pagesAdult HIV Notes On GuidelinesJokerPas encore d'évaluation
- The Life Cycle of WormsDocument5 pagesThe Life Cycle of WormsNikko AdhitamaPas encore d'évaluation
- Antigen - Antibody Reactions: Dr.D.BinduDocument46 pagesAntigen - Antibody Reactions: Dr.D.Bindubindu dhanapalPas encore d'évaluation
- Septic Shock Nursing Assessment and ManagementDocument6 pagesSeptic Shock Nursing Assessment and ManagementJenn GallowayPas encore d'évaluation
- Assistance To States For Control of Animal Diseases (ASCADDocument6 pagesAssistance To States For Control of Animal Diseases (ASCADMonal DaptardarPas encore d'évaluation
- E. faecalis Endodontic ChallengeDocument5 pagesE. faecalis Endodontic ChallengeMonica RoopChanderPas encore d'évaluation
- Feline Dermatophytosis Treatment RecommendationsDocument21 pagesFeline Dermatophytosis Treatment RecommendationsFrancisca Thenée SerranoPas encore d'évaluation
- Diphtheria, Enterobiasis, FilariasisDocument2 pagesDiphtheria, Enterobiasis, FilariasisAngel Joy CatalanPas encore d'évaluation
- Rincian Kewenangan Klinis Dokter Spesialis Anak: Congenital DisordersDocument6 pagesRincian Kewenangan Klinis Dokter Spesialis Anak: Congenital DisordersIMELDA ARCANPas encore d'évaluation
- Test Abbreviations Rev 11 24 15Document2 pagesTest Abbreviations Rev 11 24 15radbirdPas encore d'évaluation
- Miller 2000Document9 pagesMiller 2000BerryEkaPardaBancinPas encore d'évaluation
- Sars-Cov-2 (Covid 19) Detection (Qualitative) by Real Time RT PCRDocument3 pagesSars-Cov-2 (Covid 19) Detection (Qualitative) by Real Time RT PCRVedant KarnatakPas encore d'évaluation
- Anopheline Fauna, Hazaribag, JharkhandDocument4 pagesAnopheline Fauna, Hazaribag, Jharkhandmrazivbu23Pas encore d'évaluation
- Treatment Outcomes in EndodonticsDocument5 pagesTreatment Outcomes in EndodonticsVimi GeorgePas encore d'évaluation
- CSOM Retroauricular FistulaDocument151 pagesCSOM Retroauricular FistulaM.rizki DestiantoroPas encore d'évaluation
- Soal Ujian SMK KLS XiDocument67 pagesSoal Ujian SMK KLS XiSmandua Kmudaatam100% (1)
- Ap Biology CH 19 Reading GuideDocument4 pagesAp Biology CH 19 Reading Guideapi-293174360Pas encore d'évaluation