Vous aimerez peut-être aussi
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Codein InpediatricsDocument9 pagesCodein InpediatricsSenandungNacitaPas encore d'évaluation
- Mayoclinproc 86 2 013 PDFDocument12 pagesMayoclinproc 86 2 013 PDFMagdy Ali ELsherbenyPas encore d'évaluation
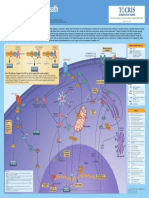
- Programmed Cell Death PosterDocument1 pageProgrammed Cell Death PosterSenandungNacitaPas encore d'évaluation
- TSQM PDFDocument13 pagesTSQM PDFSenandungNacitaPas encore d'évaluation
- Targeted Therapy Antibodi MonoklonalDocument17 pagesTargeted Therapy Antibodi MonoklonalSenandungNacitaPas encore d'évaluation
- Therapeutic Drug MonitoringDocument10 pagesTherapeutic Drug MonitoringCarina JLPas encore d'évaluation
- JP16eng PDFDocument2 326 pagesJP16eng PDFVladislav1982100% (2)
- WHO - Haemoglobin Level For Anemia 2011Document6 pagesWHO - Haemoglobin Level For Anemia 2011Adhi SanjayaPas encore d'évaluation
- Prediksi WinsaamDocument10 pagesPrediksi Winsaamsanizakkia100% (1)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Oman New Health Application FormDocument3 pagesOman New Health Application FormAravind AlavantharPas encore d'évaluation
- Detailed Lesson Plan in Quarter 4 WK 1 Digestive ProcessDocument10 pagesDetailed Lesson Plan in Quarter 4 WK 1 Digestive ProcessmalouPas encore d'évaluation
- Cronbachs AlphaDocument2 pagesCronbachs AlphaSonia Ticona BenaventePas encore d'évaluation
- Internet Book of Critical Care (IBCC) : Rapid ReferenceDocument1 pageInternet Book of Critical Care (IBCC) : Rapid Referenceian porterPas encore d'évaluation
- IV Push MedicationsDocument67 pagesIV Push Medicationsbtalera100% (1)
- Pom Maker The Ultimate Yarn Guide For Pompom MakingDocument20 pagesPom Maker The Ultimate Yarn Guide For Pompom MakingMaciek PikułaPas encore d'évaluation
- Hendra - EKGDocument34 pagesHendra - EKGRINAPas encore d'évaluation
- Medscape Physician Compensation Report 2023 - Your Income Vs Your Peers'Document8 pagesMedscape Physician Compensation Report 2023 - Your Income Vs Your Peers'David J ShinPas encore d'évaluation
- Tips in The Care and MGT of PIGS PDFDocument20 pagesTips in The Care and MGT of PIGS PDFArleo NarcisoPas encore d'évaluation
- Case Study On Observation and Newborn CareDocument38 pagesCase Study On Observation and Newborn CarePiyush Dutta100% (2)
- Pathophysiology of Respiratory Diseases: Obstructed AlveoliDocument3 pagesPathophysiology of Respiratory Diseases: Obstructed AlveoliApril Dianne ParungaoPas encore d'évaluation
- ADR UzbekistanDocument80 pagesADR UzbekistanJose Juan Velazquez GarciaPas encore d'évaluation
- PMO - Pasteurized Milk OrdinanceDocument340 pagesPMO - Pasteurized Milk OrdinanceTato G.k.Pas encore d'évaluation
- Hand When You Need Them MostDocument9 pagesHand When You Need Them MostJim SchotterPas encore d'évaluation
- Ingrown Nail RemovalDocument28 pagesIngrown Nail RemovaljaphetnwapiPas encore d'évaluation
- PEGS CatalogDocument88 pagesPEGS CatalogMPas encore d'évaluation
- Epidemiology SlidesDocument30 pagesEpidemiology SlidesHongMingPas encore d'évaluation
- 13 Levels of AssessmentDocument11 pages13 Levels of AssessmentCatherine Cayda dela Cruz-BenjaminPas encore d'évaluation
- Ebr MacalolotDocument4 pagesEbr Macalolotquen.chuaPas encore d'évaluation
- AmavataDocument14 pagesAmavataSamhitha Ayurvedic ChennaiPas encore d'évaluation
- Single Best Answer Question-Writing Tips For Clinicians: J L Walsh, B H L Harris, P E SmithDocument6 pagesSingle Best Answer Question-Writing Tips For Clinicians: J L Walsh, B H L Harris, P E SmithSandro ToninPas encore d'évaluation
- Diane Pills Drug StudyDocument4 pagesDiane Pills Drug StudyDawn EncarnacionPas encore d'évaluation
- Census August 8 - August 9, 2020Document6 pagesCensus August 8 - August 9, 2020Patrick JohnPas encore d'évaluation
- Primer: Gastro-Oesophageal Reflux DiseaseDocument23 pagesPrimer: Gastro-Oesophageal Reflux Diseasejcacia17Pas encore d'évaluation
- Poultry ParasitesDocument164 pagesPoultry ParasitesGiselle Castro Sabino100% (1)
- Tuberculosis: by Rohma XI A2, Roll No.-2Document15 pagesTuberculosis: by Rohma XI A2, Roll No.-2fur ballPas encore d'évaluation
- Dehorning DisbuddingDocument4 pagesDehorning DisbuddingAnca AnghelescuPas encore d'évaluation
- GinaDocument59 pagesGinasigitPas encore d'évaluation
- Mustang Track Loader Mtl25 Service Manual 908313 RevcDocument23 pagesMustang Track Loader Mtl25 Service Manual 908313 Revcnicoleorr110382okaPas encore d'évaluation
- The Herbal of Dioscorides Materia MedicaDocument78 pagesThe Herbal of Dioscorides Materia MedicaShari Cook100% (2)