Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Roland Barthes - Steak and ChipsDocument3 pagesRoland Barthes - Steak and ChipsmishaiolandaPas encore d'évaluation
- Most Expected Vocabulary Ebook by Prashant SirDocument35 pagesMost Expected Vocabulary Ebook by Prashant SirPriya GuptaPas encore d'évaluation
- Image of The Month: Caput MedusaeDocument1 pageImage of The Month: Caput MedusaeRoery ImoetPas encore d'évaluation
- Jurnal AnakDocument11 pagesJurnal AnakRoery ImoetPas encore d'évaluation
- Sepsis PDFDocument11 pagesSepsis PDFRoery ImoetPas encore d'évaluation
- BPH 2Document15 pagesBPH 2Roery ImoetPas encore d'évaluation
- Disaster Management Handbook: Disaster Management Cycle Hal 509 Buku Natural Disaster: Disaster Cycle Halaman 24. Buku Koenig. Disaster Cycle Halmn 8Document1 pageDisaster Management Handbook: Disaster Management Cycle Hal 509 Buku Natural Disaster: Disaster Cycle Halaman 24. Buku Koenig. Disaster Cycle Halmn 8Roery ImoetPas encore d'évaluation
- Hand Hygiene Practices: Travancore Medical College, Kollam. Kerala. IndiaDocument39 pagesHand Hygiene Practices: Travancore Medical College, Kollam. Kerala. IndiaRoery ImoetPas encore d'évaluation
- 15 33 1 SMDocument9 pages15 33 1 SMSeptin Puspita Ningrum - ArumPas encore d'évaluation
- Retention and RelapseDocument32 pagesRetention and RelapseRana SayedPas encore d'évaluation
- TCM Tongue Diagnosis - Join The RAWvolutionDocument4 pagesTCM Tongue Diagnosis - Join The RAWvolutionJing CruzPas encore d'évaluation
- Reproductive Toxicology: J.P. Klein, M. Mold, L. Mery, M. Cottier, C. ExleyDocument6 pagesReproductive Toxicology: J.P. Klein, M. Mold, L. Mery, M. Cottier, C. ExleySara BouchelouchePas encore d'évaluation
- Papular UrticariaDocument10 pagesPapular UrticariaNuri Sakina SuhartoPas encore d'évaluation
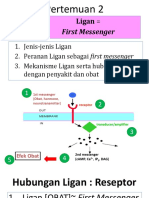
- 2 Ligan First MassengerDocument32 pages2 Ligan First MassengerikhararaPas encore d'évaluation
- RSOM Mark SchemesDocument26 pagesRSOM Mark SchemesElaine Rosemary BrucePas encore d'évaluation
- Practical PhysiologyDocument436 pagesPractical Physiologyaastha212002100% (1)
- Beneath The SurfaceDocument3 pagesBeneath The Surfacechristine_catar4736Pas encore d'évaluation
- Rat DissectionDocument5 pagesRat DissectionAcidri AbdulkarimPas encore d'évaluation
- Milia AriaDocument8 pagesMilia AriaAtsabitFarisPas encore d'évaluation
- Cholesterol PresentationDocument28 pagesCholesterol Presentationapi-240098169Pas encore d'évaluation
- Intervention For Voice Disorders PDFDocument14 pagesIntervention For Voice Disorders PDFSiti muhajarohPas encore d'évaluation
- What Is EcgDocument5 pagesWhat Is EcgLeeyan MeePas encore d'évaluation
- Practical Hematology ManualDocument48 pagesPractical Hematology ManualHaael88Pas encore d'évaluation
- Symbiosis Practice PDFDocument10 pagesSymbiosis Practice PDFMark ArcePas encore d'évaluation
- Philippine Dental Association Covid 19 Monitoring FormDocument1 pagePhilippine Dental Association Covid 19 Monitoring Formrhusolano rhusolanoPas encore d'évaluation
- Dairy FarmingDocument1 pageDairy FarmingyogasanaPas encore d'évaluation
- NCP Fdar Fin.Document8 pagesNCP Fdar Fin.Bissette DomingoPas encore d'évaluation
- Protozoa PowerpointDocument36 pagesProtozoa PowerpointHarriza Macapundag Haron-GangcoPas encore d'évaluation
- Prenatal DevelopmentDocument23 pagesPrenatal DevelopmentCelestina TanPas encore d'évaluation
- BetaStar 1206Document2 pagesBetaStar 1206api-3697331Pas encore d'évaluation
- Macro - Micronutrients and Their Sources and FunctionsDocument12 pagesMacro - Micronutrients and Their Sources and FunctionsClayohj Alliana0% (1)
- About HyenaDocument24 pagesAbout HyenaRiswan Hanafyah Harahap0% (1)
- John W. Campbell - Who Goes There-Rosettabooks (2001)Document56 pagesJohn W. Campbell - Who Goes There-Rosettabooks (2001)Manuel KlosterPas encore d'évaluation
- Karakteristik Ibu Hamil Dengan Ketuban Pecah Dini Di Rsu Assalam, Gemolong, SragenDocument7 pagesKarakteristik Ibu Hamil Dengan Ketuban Pecah Dini Di Rsu Assalam, Gemolong, SragenaniPas encore d'évaluation
- Mother's Class BFDocument55 pagesMother's Class BFriz04_fortitudessa5178Pas encore d'évaluation
- A Practicle Handbook of Dairy HusbandryDocument122 pagesA Practicle Handbook of Dairy HusbandryGian Niotis100% (1)
- Spina Bifida PresentationDocument11 pagesSpina Bifida Presentationapi-242435091Pas encore d'évaluation