Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- Primal Hormones Made by Aesthetic Primal 1Document59 pagesPrimal Hormones Made by Aesthetic Primal 1enzopark776Pas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Prenatal CardDocument2 pagesPrenatal CardMandeep SinghPas encore d'évaluation
- Sarah TalleyDocument3 pagesSarah TalleyMandeep Singh67% (3)
- Annotated Bibliography Negative Effect of Social MediaDocument6 pagesAnnotated Bibliography Negative Effect of Social MedialukmaanPas encore d'évaluation
- Tooth DecayDocument28 pagesTooth DecayRyan Carlo CondePas encore d'évaluation
- BGPDocument12 pagesBGPMandeep SinghPas encore d'évaluation
- Do Work in Health Care After AllDocument6 pagesDo Work in Health Care After AllMandeep SinghPas encore d'évaluation
- ENG Implementation Strategy IHCC Monitor CommDocument41 pagesENG Implementation Strategy IHCC Monitor CommMandeep SinghPas encore d'évaluation
- E453 PDFDocument14 pagesE453 PDFMandeep SinghPas encore d'évaluation
- Financing The Universal Access Health Care SystemDocument7 pagesFinancing The Universal Access Health Care SystemMandeep SinghPas encore d'évaluation
- The Median Sales Value Is 66.82: RM (List Ls ) Setwd ("C:/Exam") GetwdDocument2 pagesThe Median Sales Value Is 66.82: RM (List Ls ) Setwd ("C:/Exam") GetwdMandeep SinghPas encore d'évaluation
- Weaning Foods For InfantsDocument24 pagesWeaning Foods For InfantsMandeep SinghPas encore d'évaluation
- PMP Study Notes 12 - Project Procurement Management Professional Development Journey - PMP, ITIL, PHPDocument6 pagesPMP Study Notes 12 - Project Procurement Management Professional Development Journey - PMP, ITIL, PHPMandeep Singh100% (1)
- MalwarebyteDocument1 pageMalwarebyteMandeep SinghPas encore d'évaluation
- System LogDocument9 pagesSystem LogMandeep SinghPas encore d'évaluation
- House Construction Project - Risk RegisterDocument4 pagesHouse Construction Project - Risk RegisterMandeep SinghPas encore d'évaluation
- Chapter 6 Costing of Service SectorDocument7 pagesChapter 6 Costing of Service SectornidhikulkarniPas encore d'évaluation
- Escalation Matrix - 2006Document3 pagesEscalation Matrix - 2006Mandeep SinghPas encore d'évaluation
- Sop UtiDocument1 pageSop UtiMandeep SinghPas encore d'évaluation
- Dr. Jaydip Bhaumik: Curriculum VitaeDocument3 pagesDr. Jaydip Bhaumik: Curriculum VitaeBibhu KalyanPas encore d'évaluation
- Roster TemplateDocument5 pagesRoster TemplateMandeep SinghPas encore d'évaluation
- Finalcrm 170104074815Document25 pagesFinalcrm 170104074815Mandeep SinghPas encore d'évaluation
- Daniel Hloombert: Summary CompetenceDocument3 pagesDaniel Hloombert: Summary CompetenceMandeep SinghPas encore d'évaluation
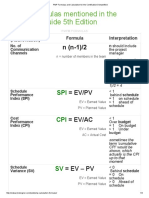
- PMP Formulas and Calculation For The Certification DemystifiedDocument4 pagesPMP Formulas and Calculation For The Certification DemystifiedMandeep SinghPas encore d'évaluation
- CRM Guide For HospitalsDocument20 pagesCRM Guide For HospitalsMandeep SinghPas encore d'évaluation
- 179 SchemaDocument1 page179 SchemaMandeep SinghPas encore d'évaluation
- PMP Study Notes 13 - Project Stakeholder Management Professional Development Journey - PMP, ITIL, PHPDocument3 pagesPMP Study Notes 13 - Project Stakeholder Management Professional Development Journey - PMP, ITIL, PHPMandeep SinghPas encore d'évaluation
- Breast Pumps Lubic Gel Xylocaine Bottle Gel Wid Ego Sterilisation List of All LabDocument1 pageBreast Pumps Lubic Gel Xylocaine Bottle Gel Wid Ego Sterilisation List of All LabMandeep SinghPas encore d'évaluation
- Bullwhip Effect SolutionsDocument1 pageBullwhip Effect SolutionsMandeep SinghPas encore d'évaluation
- Agarwal PackersDocument1 pageAgarwal PackersMandeep SinghPas encore d'évaluation
- Question Project CoordinatorDocument3 pagesQuestion Project CoordinatorMandeep SinghPas encore d'évaluation
- Escalation Matrix - 2006Document3 pagesEscalation Matrix - 2006Mandeep SinghPas encore d'évaluation
- 25 High Calorie Recipes PDFDocument14 pages25 High Calorie Recipes PDFAndrei Chirila100% (1)
- Tic-Tac-Toe Copy 1Document2 pagesTic-Tac-Toe Copy 1api-481435687Pas encore d'évaluation
- Annotated BibliographyDocument8 pagesAnnotated Bibliographyapi-282022477Pas encore d'évaluation
- Treatment in Childhood DiarrhoeaDocument17 pagesTreatment in Childhood DiarrhoeaPrabir Kumar ChatterjeePas encore d'évaluation
- DIETDocument4 pagesDIETPrabu G SatiyaPas encore d'évaluation
- How To Build Your Own Workout Routine Nerd FitnessDocument13 pagesHow To Build Your Own Workout Routine Nerd Fitnessdoc mo100% (1)
- Grade 10 ReviewerDocument6 pagesGrade 10 ReviewerJoanne JaenPas encore d'évaluation
- J1-T5 Anemia FerropénicaDocument12 pagesJ1-T5 Anemia FerropénicaGoblin HunterPas encore d'évaluation
- Bischoff 2019 - Obesity TherapyDocument10 pagesBischoff 2019 - Obesity TherapyEvania Astella SetiawanPas encore d'évaluation
- Comparison of Body Composition and Nutrients' Deficiencies Between Portuguese Rink-Hockey PlayersDocument10 pagesComparison of Body Composition and Nutrients' Deficiencies Between Portuguese Rink-Hockey PlayersNutricionista Paulo MartinsPas encore d'évaluation
- Childhood Obesity in The Rio Grande ValleyDocument6 pagesChildhood Obesity in The Rio Grande ValleydjwickedPas encore d'évaluation
- Armadillo Meerkat NarwhalDocument16 pagesArmadillo Meerkat Narwhalganeshthangam.e3324Pas encore d'évaluation
- Ismenore: You Should Also DoDocument2 pagesIsmenore: You Should Also DoNurul Ilmi UtamiPas encore d'évaluation
- DM Type II Case StudyDocument28 pagesDM Type II Case StudyRichard Sy67% (3)
- Pud Case StudyDocument8 pagesPud Case Studyapi-346620455Pas encore d'évaluation
- Mr. Olympia: Nutrition GuideDocument11 pagesMr. Olympia: Nutrition GuideAkul Chauhan100% (1)
- Overripe Banana SweetenerDocument5 pagesOverripe Banana SweetenerJulieann YacubPas encore d'évaluation
- Guide in Making The CreedDocument2 pagesGuide in Making The CreedLaedyn Faye IsipPas encore d'évaluation
- Lightweight Rowers. Seasonal Variations in The Body Composition ofDocument5 pagesLightweight Rowers. Seasonal Variations in The Body Composition ofGizem OzkayaPas encore d'évaluation
- The Art of Raw Food Paulina Nienartowicz EbookDocument104 pagesThe Art of Raw Food Paulina Nienartowicz EbookcecyromanoPas encore d'évaluation
- The Rainbow Diet Recipe EBooklet HRDocument12 pagesThe Rainbow Diet Recipe EBooklet HRекатерина100% (1)
- ButterDocument31 pagesButterLe HuyPas encore d'évaluation
- Clinical Screening Form - AgriSafe NetworkDocument4 pagesClinical Screening Form - AgriSafe NetworkAgriSafePas encore d'évaluation
- Grade 6 NutritionDocument5 pagesGrade 6 NutritionCristina RăileanuPas encore d'évaluation
- Sugar Film Movie ReviewDocument2 pagesSugar Film Movie ReviewJocel VictoriaPas encore d'évaluation
- TSA EpidermidisDocument2 pagesTSA EpidermidisVi Vian HiuPas encore d'évaluation
- Top 10 Foods For EyesightDocument8 pagesTop 10 Foods For EyesightIndah WulandariPas encore d'évaluation