Vous aimerez peut-être aussi
- Heal Yourself-The Natural WayDocument489 pagesHeal Yourself-The Natural Waygemoregold100% (18)
- History and Mental Status Exam GuideDocument17 pagesHistory and Mental Status Exam Guideyeney armenterosPas encore d'évaluation
- Pneumonia Cheat Sheet: by ViaDocument3 pagesPneumonia Cheat Sheet: by ViaGayle MariePas encore d'évaluation
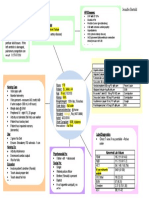
- Concept Map HypertensionDocument1 pageConcept Map Hypertensiongeorge pearson0% (1)
- Completed Concept MapDocument4 pagesCompleted Concept Mapapi-607361848Pas encore d'évaluation
- System Disorder: Renal CalculiDocument1 pageSystem Disorder: Renal CalculiHolly DeckelmanPas encore d'évaluation
- Physical AssessmentDocument3 pagesPhysical AssessmentHyacinth ExmundoPas encore d'évaluation
- Basic Tools in NutritionDocument23 pagesBasic Tools in NutritionSeanmarie Cabrales0% (1)
- Concept MapDocument5 pagesConcept Mapapi-546509005Pas encore d'évaluation
- Quotes NursingDocument14 pagesQuotes NursingFreddy ÁlvaroPas encore d'évaluation
- Description: Congestive Heart FailureDocument22 pagesDescription: Congestive Heart FailurePinklet Arleena CubianPas encore d'évaluation
- 5P Handoff SheetDocument1 page5P Handoff SheetBarry SeeboPas encore d'évaluation
- Nursing AssessmentDocument16 pagesNursing AssessmentJihan Novita100% (1)
- Head to-Toe-Assessment Complete Guide - Nightingale CollegeDocument1 pageHead to-Toe-Assessment Complete Guide - Nightingale CollegeDabon RusselPas encore d'évaluation
- Fluidsandelectrolytes 090224074347 Phpapp02Document102 pagesFluidsandelectrolytes 090224074347 Phpapp02IsaacJ22Pas encore d'évaluation
- Stroke Signs, Risks, and Nursing CareDocument1 pageStroke Signs, Risks, and Nursing CareMariel Febreo MerlanPas encore d'évaluation
- Case Simu 101Document5 pagesCase Simu 101Princess Levie CenizaPas encore d'évaluation
- Legal/Forensic Medicine: Atty. Tony D. Rebosa, MD, BscrimDocument30 pagesLegal/Forensic Medicine: Atty. Tony D. Rebosa, MD, BscrimAlpana Laisom75% (4)
- Concept Map 2Document1 pageConcept Map 2lanrevoicePas encore d'évaluation
- Medical Surgical Nursing IIDocument52 pagesMedical Surgical Nursing IItwinkle143Pas encore d'évaluation
- Appendix 10 Patient Profile TemplateDocument6 pagesAppendix 10 Patient Profile TemplateAL Rizwan AsifPas encore d'évaluation
- Diabetes Mellitus Complte LONG 2Document56 pagesDiabetes Mellitus Complte LONG 2John Vincent Dy OcampoPas encore d'évaluation
- Diabetes Mellitus Complte LONG 2Document56 pagesDiabetes Mellitus Complte LONG 2John Vincent Dy OcampoPas encore d'évaluation
- Prof. Sandra M. Covarrubias - September 24, 2021: 5.2fluid & Electrolytes ImbalancesDocument5 pagesProf. Sandra M. Covarrubias - September 24, 2021: 5.2fluid & Electrolytes ImbalancesIvy VillalobosPas encore d'évaluation
- Educational Strategies For Children With Emotional and Behavioral ProblemsDocument74 pagesEducational Strategies For Children With Emotional and Behavioral Problemsmaeydel50% (2)
- Pediatric Concept MapDocument12 pagesPediatric Concept Mapapi-352157080Pas encore d'évaluation
- Care of Pediatric Client With Dermatologic DisorderDocument3 pagesCare of Pediatric Client With Dermatologic DisorderAraw GabiPas encore d'évaluation
- System Disorder ADDocument1 pageSystem Disorder ADSariahPas encore d'évaluation
- Waiters Rhabdomyolysis PDFDocument1 pageWaiters Rhabdomyolysis PDFmp1757Pas encore d'évaluation
- Pico Question WatchornDocument5 pagesPico Question Watchornapi-301725567Pas encore d'évaluation
- POC and Concepts Maps Week 12Document23 pagesPOC and Concepts Maps Week 12Michelle CollinsPas encore d'évaluation
- ACTIVE LEARNING TEMPLATE: System DisorderDocument1 pageACTIVE LEARNING TEMPLATE: System DisorderDeo FactuarPas encore d'évaluation
- Immersion Physical Exam Final - ChecklistDocument2 pagesImmersion Physical Exam Final - ChecklistElizalde HusbandPas encore d'évaluation
- Concept Map Meningitis TheoryDocument3 pagesConcept Map Meningitis TheoryMia AuliaPas encore d'évaluation
- Week 7 - Rheumatoid ArthritisDocument1 pageWeek 7 - Rheumatoid ArthritisTuTitPas encore d'évaluation
- Renal Concept MapDocument1 pageRenal Concept MapShaira Ann CalambaPas encore d'évaluation
- Newborn Care PDFDocument8 pagesNewborn Care PDFZedrake CaraanPas encore d'évaluation
- Acute and Chronic GastritisDocument6 pagesAcute and Chronic GastritisAnn CanPas encore d'évaluation
- Potential Complications Signs and SymptomsDocument2 pagesPotential Complications Signs and SymptomsJessica GomezPas encore d'évaluation
- CHF Concept MapDocument1 pageCHF Concept MapChristy Wegner Cooper100% (4)
- Nursing Care Plan for Patient with Gastric CancerDocument7 pagesNursing Care Plan for Patient with Gastric CancerHilario. Hayascent.Reign.M.Pas encore d'évaluation
- Concept Map 360Document6 pagesConcept Map 360api-273469220Pas encore d'évaluation
- Leoprolide Drug StudyDocument2 pagesLeoprolide Drug Studyhappymee927Pas encore d'évaluation
- Vancomycin Dosing and Monitoring in AdultsDocument1 pageVancomycin Dosing and Monitoring in AdultsjulialeoPas encore d'évaluation
- ATI Medication TemplateDocument1 pageATI Medication Templatephoenix180Pas encore d'évaluation
- Generic and Trade Names, Mechanisms, InterventionsDocument4 pagesGeneric and Trade Names, Mechanisms, InterventionsSonia FernandesPas encore d'évaluation
- Community Health Nursing Lecture: Family Health AssessmentDocument7 pagesCommunity Health Nursing Lecture: Family Health AssessmentSofia ResolPas encore d'évaluation
- Abdominal Assessment VideoDocument4 pagesAbdominal Assessment VideoAmber Nicole HubbardPas encore d'évaluation
- IVY TECH NURSING LAB INFORMATIONDocument7 pagesIVY TECH NURSING LAB INFORMATIONSethPas encore d'évaluation
- Teamworks! Game: Summary ReportDocument2 pagesTeamworks! Game: Summary ReportAngela May Pustasa AllamPas encore d'évaluation
- Fluids Electrolytes Visual NotesDocument8 pagesFluids Electrolytes Visual NotesVin Lorenzo CampbellPas encore d'évaluation
- Idiopathic Thrombocytopenic Purpura: Overview With Report of A CaseDocument4 pagesIdiopathic Thrombocytopenic Purpura: Overview With Report of A CaseHernan GonzalezPas encore d'évaluation
- Part I: Emergency Department (ED) : SKINNY ReasoningDocument6 pagesPart I: Emergency Department (ED) : SKINNY ReasoningUzumaki KPas encore d'évaluation
- DRUG STUDY FINAL (Onco) PDFDocument14 pagesDRUG STUDY FINAL (Onco) PDFFrancis Anthony LoslosoPas encore d'évaluation
- Medication - ALT-Template Polythene GlycolDocument1 pageMedication - ALT-Template Polythene GlycolNancyAmissahPas encore d'évaluation
- Care Plan FaringitisDocument63 pagesCare Plan FaringitisEnerolisa ParedesPas encore d'évaluation
- Case Study 101: Abdominal Aortic Aneurysm With Acute Kidney InjuryDocument8 pagesCase Study 101: Abdominal Aortic Aneurysm With Acute Kidney InjuryPatricia Ann Nicole ReyesPas encore d'évaluation
- IWU Nursing Care Plan for 81-Year-Old Female with CHF and PneumoniaDocument6 pagesIWU Nursing Care Plan for 81-Year-Old Female with CHF and PneumoniaclarimerPas encore d'évaluation
- Behavioral Health Care PlanDocument12 pagesBehavioral Health Care Planapi-520841770100% (1)
- Nursing Care Plan: Assessment Diagnosis Inference Planning Intervention Rationale EvaluationDocument3 pagesNursing Care Plan: Assessment Diagnosis Inference Planning Intervention Rationale EvaluationJessa FabicoPas encore d'évaluation
- Data Collection and Patient DiagnosisDocument14 pagesData Collection and Patient DiagnosisJen CareyPas encore d'évaluation
- GRP 4 CLO 2 Concept Map PT 1 PDFDocument14 pagesGRP 4 CLO 2 Concept Map PT 1 PDFMaria Lyn Ocariza ArandiaPas encore d'évaluation
- ClindamycinDocument3 pagesClindamycinShaira TanPas encore d'évaluation
- Nursing Process Overview: Health Assessment NotesDocument40 pagesNursing Process Overview: Health Assessment NotesEliakim III InsongPas encore d'évaluation
- NANDA Nursing DiagnosesDocument8 pagesNANDA Nursing DiagnosesShreejana PrajapatiPas encore d'évaluation
- NURSING CARE OF ADULTS II: Passbooks Study GuideD'EverandNURSING CARE OF ADULTS II: Passbooks Study GuidePas encore d'évaluation
- COMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideD'EverandCOMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuidePas encore d'évaluation
- Guidance on Evaluating and Treating UTIs and ASBDocument14 pagesGuidance on Evaluating and Treating UTIs and ASBJohn Vincent Dy OcampoPas encore d'évaluation
- Renal TuberculosisDocument43 pagesRenal TuberculosisPulse OfMedicoPas encore d'évaluation
- Pediatric Community-Acquired Pneumonia Clinical Guideline PDFDocument1 pagePediatric Community-Acquired Pneumonia Clinical Guideline PDFJohn Vincent Dy OcampoPas encore d'évaluation
- Manajemen Sepsis - SSCDocument8 pagesManajemen Sepsis - SSCDeborah Bravian TairasPas encore d'évaluation
- AcuteCoronary SyndromesDocument108 pagesAcuteCoronary SyndromesJohn Vincent Dy OcampoPas encore d'évaluation
- Chapter 95 Complications of Urologic Procedures and DevicesDocument39 pagesChapter 95 Complications of Urologic Procedures and DevicesJohn Vincent Dy OcampoPas encore d'évaluation
- Quality Sepsis Definitions SCCM ESICM Joint Session Critical Care CongressDocument88 pagesQuality Sepsis Definitions SCCM ESICM Joint Session Critical Care CongressSandritaAquinoPas encore d'évaluation
- Clinical Trials PhasesDocument2 pagesClinical Trials PhasespandabijoyPas encore d'évaluation
- Cap Guidelines Booklet 2010 UpdateDocument101 pagesCap Guidelines Booklet 2010 UpdateIcko DinopolPas encore d'évaluation
- Lower Respiratory Tract InfectionDocument21 pagesLower Respiratory Tract InfectionJohn Vincent Dy OcampoPas encore d'évaluation
- A LilingDocument3 pagesA LilingJohn Vincent Dy OcampoPas encore d'évaluation
- SCSD Application Summary Form PDFDocument2 pagesSCSD Application Summary Form PDFJoserie HernanePas encore d'évaluation
- Beat COVID-19 Situationer #004 (May 1)Document9 pagesBeat COVID-19 Situationer #004 (May 1)Glomarie Alyssa RacelisPas encore d'évaluation
- Basics of Critical Care.....Document34 pagesBasics of Critical Care.....XamanPas encore d'évaluation
- Physio Assess Form Oct 2022Document5 pagesPhysio Assess Form Oct 2022RishaadPas encore d'évaluation
- Handwashing NarrativeDocument9 pagesHandwashing NarrativeMaria Angelica BermilloPas encore d'évaluation
- Ovr New MohDocument2 pagesOvr New MohhyPas encore d'évaluation
- 243 471 1 SM PDFDocument6 pages243 471 1 SM PDFFia lutfiahPas encore d'évaluation
- En - 2316 9117 FP 26 04 380Document14 pagesEn - 2316 9117 FP 26 04 380Ana paula CamargoPas encore d'évaluation
- Estradiol 1mg + Norethisterone Acetate 0.5mg (Activelle)Document12 pagesEstradiol 1mg + Norethisterone Acetate 0.5mg (Activelle)asdwasdPas encore d'évaluation
- Faculty of Sport Science and Recreation Diploma in Sport Studies (Sr1132D) Sps220 - Nutrition For Health and ExerciseDocument6 pagesFaculty of Sport Science and Recreation Diploma in Sport Studies (Sr1132D) Sps220 - Nutrition For Health and ExerciseSyafiq MiqhaelPas encore d'évaluation
- INITIAL DATA BASE Form For Family 1Document5 pagesINITIAL DATA BASE Form For Family 1Reignallienn Inocencio MartinPas encore d'évaluation
- Efudix Leaflet With PicturesDocument2 pagesEfudix Leaflet With PicturesyehyaPas encore d'évaluation
- Database Clerk Vacancy in MawlamyineDocument3 pagesDatabase Clerk Vacancy in MawlamyineHein Min NaingPas encore d'évaluation
- 5ОМ англ ВОП 1Document22 pages5ОМ англ ВОП 1p69b24hy8pPas encore d'évaluation
- Renal Colic and Joint DeformitiesDocument19 pagesRenal Colic and Joint DeformitiesAhmad Syahmi YZ100% (1)
- Careers in Social Work: Outlook, Pay & MoreDocument9 pagesCareers in Social Work: Outlook, Pay & Morejoel lacayPas encore d'évaluation
- 4 Coercion in Mental Healthcare The Principle of Least Coercive CareDocument8 pages4 Coercion in Mental Healthcare The Principle of Least Coercive CarePedro Y. LuyoPas encore d'évaluation
- Mammograms and Other Breast Imaging Procedures: What Is A Mammogram?Document25 pagesMammograms and Other Breast Imaging Procedures: What Is A Mammogram?Marina StosicPas encore d'évaluation
- PHARMACOLOGY PrelimDocument26 pagesPHARMACOLOGY PrelimCrystal MiranaPas encore d'évaluation
- Dme Information Form Cms-10125 - External Infusion PumpsDocument2 pagesDme Information Form Cms-10125 - External Infusion PumpsSonof GoddPas encore d'évaluation
- STRDocument179 pagesSTRJatin AnandPas encore d'évaluation
- Konsult Sip ReportDocument72 pagesKonsult Sip ReportMohit AgarwalPas encore d'évaluation
- Cook 2009 Oropharyngeal DysphagiaDocument21 pagesCook 2009 Oropharyngeal DysphagiaDesiré MagalhãesPas encore d'évaluation
- Exams NAC Guideline Rating Scale PDFDocument2 pagesExams NAC Guideline Rating Scale PDFprakash13lPas encore d'évaluation
- HIV Testing and Management in IndonesiaDocument31 pagesHIV Testing and Management in IndonesiayurdiansyahPas encore d'évaluation