Vous aimerez peut-être aussi
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- Adult Echocardiography Protocol 14 2Document10 pagesAdult Echocardiography Protocol 14 2api-349402240Pas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- 2nd Trimester Protocol r14 PDFDocument8 pages2nd Trimester Protocol r14 PDFapi-390240132Pas encore d'évaluation
- Using MonteCarlo Simulation To Mitigate The Risk of Project Cost OverrunsDocument8 pagesUsing MonteCarlo Simulation To Mitigate The Risk of Project Cost OverrunsJancarlo Mendoza MartínezPas encore d'évaluation
- Dekker V Weida Amicus Brief by 17 AGsDocument35 pagesDekker V Weida Amicus Brief by 17 AGsSarah WeaverPas encore d'évaluation
- Corporate Members List Iei Mysore Local CentreDocument296 pagesCorporate Members List Iei Mysore Local CentreNagarjun GowdaPas encore d'évaluation
- Physics I 2016 SyllabusDocument9 pagesPhysics I 2016 SyllabusLovely SaintsPas encore d'évaluation
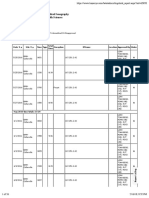
- HTTPS:WWW - Trajecsys.com:beta:ev Report - Aspx?toggle Labels&eid 3223Document2 pagesHTTPS:WWW - Trajecsys.com:beta:ev Report - Aspx?toggle Labels&eid 3223Lovely SaintsPas encore d'évaluation
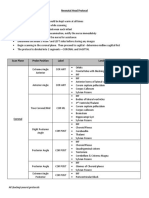
- Neonatal Head Protocol 14Document5 pagesNeonatal Head Protocol 14Lovely SaintsPas encore d'évaluation
- Time TotalsDocument26 pagesTime TotalsLovely SaintsPas encore d'évaluation
- Exams RecordsDocument2 pagesExams RecordsLovely SaintsPas encore d'évaluation
- Julia Santos, RDMS: 1677 Forsythe Trail, Collierville, Tennessee 38017Document2 pagesJulia Santos, RDMS: 1677 Forsythe Trail, Collierville, Tennessee 38017Lovely SaintsPas encore d'évaluation
- Katie - Cody@bchs - Edu: Course Syllabus Subject To ChangeDocument16 pagesKatie - Cody@bchs - Edu: Course Syllabus Subject To ChangeLovely SaintsPas encore d'évaluation
- Julia Santos: 1677 Forsythe Trail, Collierville, Tennessee 38017Document2 pagesJulia Santos: 1677 Forsythe Trail, Collierville, Tennessee 38017Lovely SaintsPas encore d'évaluation
- Quantification Group ProjectDocument29 pagesQuantification Group ProjectLovely SaintsPas encore d'évaluation
- Fetal Heart ProjectDocument10 pagesFetal Heart ProjectLovely SaintsPas encore d'évaluation
- Santos CME Cert 1Document1 pageSantos CME Cert 1Lovely SaintsPas encore d'évaluation
- Santos CME Cert 1Document1 pageSantos CME Cert 1Lovely SaintsPas encore d'évaluation
- Panc Paper SU17Document8 pagesPanc Paper SU17Lovely SaintsPas encore d'évaluation
- Interpersonal Assignment RadDocument2 pagesInterpersonal Assignment RadLovely SaintsPas encore d'évaluation
- OB Presentation SU17Document15 pagesOB Presentation SU17Lovely SaintsPas encore d'évaluation
- Julia Santos: 1677 Forsythe Trail, Collierville, Tennessee 38017Document2 pagesJulia Santos: 1677 Forsythe Trail, Collierville, Tennessee 38017Lovely SaintsPas encore d'évaluation
- 7540 Physics Question Paper 1 Jan 2011Document20 pages7540 Physics Question Paper 1 Jan 2011abdulhadii0% (1)
- Northern Lights - 7 Best Places To See The Aurora Borealis in 2022Document15 pagesNorthern Lights - 7 Best Places To See The Aurora Borealis in 2022labendetPas encore d'évaluation
- LNWH Alcohol GUIDELINE SUMMARY 2018Document1 pageLNWH Alcohol GUIDELINE SUMMARY 2018Ai Hwa LimPas encore d'évaluation
- Student Committee Sma Al Abidin Bilingual Boarding School: I. BackgroundDocument5 pagesStudent Committee Sma Al Abidin Bilingual Boarding School: I. BackgroundAzizah Bilqis ArroyanPas encore d'évaluation
- EQUIP9-Operations-Use Case ChallengeDocument6 pagesEQUIP9-Operations-Use Case ChallengeTushar ChaudhariPas encore d'évaluation
- Chapter 8 - Current Electricity - Selina Solutions Concise Physics Class 10 ICSE - KnowledgeBoatDocument123 pagesChapter 8 - Current Electricity - Selina Solutions Concise Physics Class 10 ICSE - KnowledgeBoatskjPas encore d'évaluation
- A Meta Analysis of The Relative Contribution of Leadership Styles To Followers Mental HealthDocument18 pagesA Meta Analysis of The Relative Contribution of Leadership Styles To Followers Mental HealthOnii ChanPas encore d'évaluation
- JLPT Application Form Method-December 2023Document3 pagesJLPT Application Form Method-December 2023Sajiri KamatPas encore d'évaluation
- 2015 Grade 4 English HL Test MemoDocument5 pages2015 Grade 4 English HL Test MemorosinaPas encore d'évaluation
- 3-CHAPTER-1 - Edited v1Document32 pages3-CHAPTER-1 - Edited v1Michael Jaye RiblezaPas encore d'évaluation
- How Do I Predict Event Timing Saturn Nakshatra PDFDocument5 pagesHow Do I Predict Event Timing Saturn Nakshatra PDFpiyushPas encore d'évaluation
- Quadratic SDocument20 pagesQuadratic SAnubastPas encore d'évaluation
- Submitted By: S.M. Tajuddin Group:245Document18 pagesSubmitted By: S.M. Tajuddin Group:245KhurshidbuyamayumPas encore d'évaluation
- List of Practicals Class Xii 2022 23Document1 pageList of Practicals Class Xii 2022 23Night FuryPas encore d'évaluation
- Water Flow Meter TypesDocument2 pagesWater Flow Meter TypesMohamad AsrulPas encore d'évaluation
- Advantages of The CapmDocument3 pagesAdvantages of The Capmdeeparaghu6Pas encore d'évaluation
- Facts About The TudorsDocument3 pagesFacts About The TudorsRaluca MuresanPas encore d'évaluation
- Design and Analysis of DC-DC Boost Converter: September 2016Document5 pagesDesign and Analysis of DC-DC Boost Converter: September 2016Anonymous Vfp0ztPas encore d'évaluation
- Description About Moon: Earth SatelliteDocument6 pagesDescription About Moon: Earth SatellitePurva KhatriPas encore d'évaluation
- Technology in Society: SciencedirectDocument10 pagesTechnology in Society: SciencedirectVARGAS MEDINA ALEJANDRAPas encore d'évaluation
- Mystakidis2022 MetaverseDocument13 pagesMystakidis2022 MetaverseVennela NandikondaPas encore d'évaluation
- Standalone Financial Results, Limited Review Report For December 31, 2016 (Result)Document4 pagesStandalone Financial Results, Limited Review Report For December 31, 2016 (Result)Shyam SunderPas encore d'évaluation
- 02 Laboratory Exercise 1Document2 pages02 Laboratory Exercise 1Mico Bryan BurgosPas encore d'évaluation
- MGT403 Slide All ChaptersDocument511 pagesMGT403 Slide All Chaptersfarah aqeelPas encore d'évaluation
- Nugent 2010 Chapter 3Document13 pagesNugent 2010 Chapter 3Ingrid BobosPas encore d'évaluation
- Duties and Responsibilities - Filipino DepartmentDocument2 pagesDuties and Responsibilities - Filipino DepartmentEder Aguirre Capangpangan100% (2)
- Angeles City National Trade SchoolDocument7 pagesAngeles City National Trade Schooljoyceline sarmientoPas encore d'évaluation