Vous aimerez peut-être aussi
- Effect of Treadmill Exercise Training On VO Peak in Chronic Obstructive Pulmonary DiseaseDocument7 pagesEffect of Treadmill Exercise Training On VO Peak in Chronic Obstructive Pulmonary DiseaseAqila Zefanya AriefmanPas encore d'évaluation
- Art:10.1007/s00540 012 1411 9Document6 pagesArt:10.1007/s00540 012 1411 9Debi SumarliPas encore d'évaluation
- Art:10.1186/1465 9921 7 127Document7 pagesArt:10.1186/1465 9921 7 127dvenumohanPas encore d'évaluation
- Arm 90 00027Document9 pagesArm 90 00027Ria RioPas encore d'évaluation
- Arm Exercise and Hyperinflation in Patients With COPD : Effect of Arm TrainingDocument8 pagesArm Exercise and Hyperinflation in Patients With COPD : Effect of Arm TrainingNaomiFettyPas encore d'évaluation
- Body Composition Markers in Older Persons With COPD: A M A, A F, L S, V B, C M, A C, A C, E E. G, F LDocument6 pagesBody Composition Markers in Older Persons With COPD: A M A, A F, L S, V B, C M, A C, A C, E E. G, F Lpina distefanoPas encore d'évaluation
- Alemayehu Et Al., (2018) Three Weeks of RespiratoryDocument14 pagesAlemayehu Et Al., (2018) Three Weeks of RespiratoryAna Flávia SordiPas encore d'évaluation
- Anand Evidence BasedDocument7 pagesAnand Evidence Based9724Pas encore d'évaluation
- Effects of Imposed Pursed-Lips Breathing On Respiratory Mechanics and Dyspnea at Rest and During Exercise in COPDDocument11 pagesEffects of Imposed Pursed-Lips Breathing On Respiratory Mechanics and Dyspnea at Rest and During Exercise in COPDGaoudam NatarajanPas encore d'évaluation
- Buchheit - Cardioespiratory and Autonomic Responses To 30-15 IFT - in Press JSCRDocument26 pagesBuchheit - Cardioespiratory and Autonomic Responses To 30-15 IFT - in Press JSCRmerlorodrPas encore d'évaluation
- Th. Wanke, D. Formanek, H. Lahrmann, H. Brath, M. Wild, Ch. Wagner, H. ZwickDocument7 pagesTh. Wanke, D. Formanek, H. Lahrmann, H. Brath, M. Wild, Ch. Wagner, H. Zwickrodrigokine777Pas encore d'évaluation
- One Minute STST Vs 6MWT en EPOCDocument10 pagesOne Minute STST Vs 6MWT en EPOCMaxi BoniniPas encore d'évaluation
- Hakala2000 PDFDocument7 pagesHakala2000 PDFVanshika GuptaPas encore d'évaluation
- Energy Expenditure 2006Document7 pagesEnergy Expenditure 2006Niar MarhaliPas encore d'évaluation
- End Inspiratory Pause Prolongation in ARDSDocument8 pagesEnd Inspiratory Pause Prolongation in ARDSMaxi BoniniPas encore d'évaluation
- Contin Educ Anaesth Crit Care Pain-2010-Agnew-33-7Document5 pagesContin Educ Anaesth Crit Care Pain-2010-Agnew-33-7deadbysunriseePas encore d'évaluation
- Jurnal COPDDocument8 pagesJurnal COPDAyahnya RafliPas encore d'évaluation
- Jurnal CopdDocument11 pagesJurnal Copdgemarawan abadiPas encore d'évaluation
- Paper 2 FranjaDocument10 pagesPaper 2 FranjaNicolás Celis MonroyPas encore d'évaluation
- Applsci 09 02842 PDFDocument13 pagesApplsci 09 02842 PDFFelicia SutarliPas encore d'évaluation
- The Lactate and Ventilatory Thresholds in Resistance TrainingDocument7 pagesThe Lactate and Ventilatory Thresholds in Resistance TrainingAntonioPas encore d'évaluation
- Physiology and Clinical Aplicattions of CPT. TCNA 2013Document13 pagesPhysiology and Clinical Aplicattions of CPT. TCNA 2013Javier VegaPas encore d'évaluation
- Dpoc 2Document7 pagesDpoc 2glaysonvelPas encore d'évaluation
- Corn OloDocument8 pagesCorn OloCristian Retamal ValderramaPas encore d'évaluation
- 293 FullDocument4 pages293 FullAldo AtjehPas encore d'évaluation
- Cardiopulmonary Exercise Testing in Patients With Liver CirrhosisDocument4 pagesCardiopulmonary Exercise Testing in Patients With Liver Cirrhosistengku zadeqPas encore d'évaluation
- Aerobic Exercise Boosts Lung FunctionDocument6 pagesAerobic Exercise Boosts Lung FunctionajenggayatriPas encore d'évaluation
- Body Position Influences The Maximum Inspiratory and Expiratory Mouth Pressures of Young Healthy SubjectsDocument3 pagesBody Position Influences The Maximum Inspiratory and Expiratory Mouth Pressures of Young Healthy SubjectsJoecoPas encore d'évaluation
- Long Term Impact Preoperator...Document6 pagesLong Term Impact Preoperator...nistormaria492Pas encore d'évaluation
- PHY2 8 E14455Document14 pagesPHY2 8 E14455Alexis Arce AlvarezPas encore d'évaluation
- Aerobic High-Intensity Intervals Improve 07Document7 pagesAerobic High-Intensity Intervals Improve 07Lindsay OrtizPas encore d'évaluation
- Indirect Calorimetry Research Tool or Essential Equipment 1Document4 pagesIndirect Calorimetry Research Tool or Essential Equipment 1CamiloAndresRinconYPas encore d'évaluation
- VonbankDocument7 pagesVonbanklsales1986oliPas encore d'évaluation
- Helgerund (Estudio Intervalos)Document7 pagesHelgerund (Estudio Intervalos)Andres PdrejnPas encore d'évaluation
- 1 s2.0 S0147956316301601 MainDocument7 pages1 s2.0 S0147956316301601 MainAna Paula BarbosaPas encore d'évaluation
- Correction Factors in METs ObeseDocument5 pagesCorrection Factors in METs ObeseFranco Marin MUñozPas encore d'évaluation
- Pone 0257595Document14 pagesPone 0257595Zulfah MidahPas encore d'évaluation
- Ejercicio DiafragmaticoDocument3 pagesEjercicio DiafragmaticoN onlyPas encore d'évaluation
- 4-Metre Gait Speed As A Functional Outcome Measure in Patients With Chronic Obstructive Pulmonary Disease (COPD)Document3 pages4-Metre Gait Speed As A Functional Outcome Measure in Patients With Chronic Obstructive Pulmonary Disease (COPD)samudraandiPas encore d'évaluation
- Medi 99 E23646Document8 pagesMedi 99 E23646panumatkhamphiranonPas encore d'évaluation
- 1 s2.0 S0954611113000620 MainDocument8 pages1 s2.0 S0954611113000620 MainNut RonakritPas encore d'évaluation
- The Effectsof Diaphragmatic Breathingand Omeprazoleon Respiratory Indicesand Diaphragmatic Excursionin Patientswith Gastroesophageal Reflux DiseaseDocument6 pagesThe Effectsof Diaphragmatic Breathingand Omeprazoleon Respiratory Indicesand Diaphragmatic Excursionin Patientswith Gastroesophageal Reflux DiseaseSHAFANA PUTRI -Pas encore d'évaluation
- Wasserman Chest 1997Document13 pagesWasserman Chest 1997Filip BreskvarPas encore d'évaluation
- Exercise-Induced Airway Obstruction in Young Asmathics Measured by IOSDocument7 pagesExercise-Induced Airway Obstruction in Young Asmathics Measured by IOSthiago gibsonPas encore d'évaluation
- Decrease in Paco2 With Prone Position Is Predictive of Improved Outcome in Acute Respiratory Distress SyndromeDocument7 pagesDecrease in Paco2 With Prone Position Is Predictive of Improved Outcome in Acute Respiratory Distress SyndromedarwigPas encore d'évaluation
- Jurnal Massa Bebas LemakDocument10 pagesJurnal Massa Bebas Lemakmona nurdin nurdinPas encore d'évaluation
- Copd 10 1703Document7 pagesCopd 10 1703brikitabelaPas encore d'évaluation
- Copd 10 1703Document7 pagesCopd 10 1703Maria Camila SanabriaPas encore d'évaluation
- Effects of training on breathing in COPDDocument4 pagesEffects of training on breathing in COPDCristian FerradaPas encore d'évaluation
- Epoc 3Document6 pagesEpoc 3Javier Enrique Barrera PachecoPas encore d'évaluation
- Crosstalk Proposal: High Intensity Interval Training Does Have A Role in Risk Reduction or Treatment of DiseaseDocument3 pagesCrosstalk Proposal: High Intensity Interval Training Does Have A Role in Risk Reduction or Treatment of Diseaseapi-298930008Pas encore d'évaluation
- Acute Resistance Exercise With Blood Flow Restriction Effects On Heart Rate, Double Product, Oxygen Saturation and Perceived ExertionDocument7 pagesAcute Resistance Exercise With Blood Flow Restriction Effects On Heart Rate, Double Product, Oxygen Saturation and Perceived ExertionJuanfran Montesinos GarciaPas encore d'évaluation
- Dead Space Analysis at Different Levels of Positive End-Expiratory Pressure in Acute Respiratory Distress Syndrome Patients. JCC 2018Document8 pagesDead Space Analysis at Different Levels of Positive End-Expiratory Pressure in Acute Respiratory Distress Syndrome Patients. JCC 2018Emiliano GogniatPas encore d'évaluation
- BODEXDocument8 pagesBODEXLindsey KaufmanPas encore d'évaluation
- Acute Response of Serum Leptin To Short Single Bout Exercise in Patients With Moderate AsthmaDocument8 pagesAcute Response of Serum Leptin To Short Single Bout Exercise in Patients With Moderate AsthmaOpenaccess Research paperPas encore d'évaluation
- Copd 10 1787Document14 pagesCopd 10 1787YOBEL NATHANIELPas encore d'évaluation
- Editorial Amato!! RC 2022Document4 pagesEditorial Amato!! RC 2022Emiliano GogniatPas encore d'évaluation
- Early Pulmonary Rehabilitation After Acute Exacerbation of COPDDocument10 pagesEarly Pulmonary Rehabilitation After Acute Exacerbation of COPDLili MorgadoPas encore d'évaluation
- Respiratory Monitoring in Mechanical Ventilation: Techniques and ApplicationsD'EverandRespiratory Monitoring in Mechanical Ventilation: Techniques and ApplicationsJian-Xin ZhouPas encore d'évaluation
- Exercise Physiology for the Pediatric and Congenital CardiologistD'EverandExercise Physiology for the Pediatric and Congenital CardiologistPas encore d'évaluation
- Knee - ProtocolDocument7 pagesKnee - ProtocolIra IraPas encore d'évaluation
- Physical Inactivity: Associated Diseases and Disorders: ReviewDocument18 pagesPhysical Inactivity: Associated Diseases and Disorders: ReviewJuan Pablo Casanova AnguloPas encore d'évaluation
- Nuffield Orthopaedic Centre NHS Trust: Delivering ExcellenceDocument28 pagesNuffield Orthopaedic Centre NHS Trust: Delivering ExcellenceMDPas encore d'évaluation
- Knee - TKR ProtocolDocument3 pagesKnee - TKR ProtocolJuan Pablo Casanova AnguloPas encore d'évaluation
- Astorino 2017Document11 pagesAstorino 2017Juan Pablo Casanova AnguloPas encore d'évaluation
- 10 1111@j 1600-0838 2012 01489 XDocument7 pages10 1111@j 1600-0838 2012 01489 XJuan Pablo Casanova AnguloPas encore d'évaluation
- Prediction of Peak Oxygen Uptake From Ratings of Perceived Exertion During A Sub-Maximal Cardiopulmonary Exercise Test in Patients With Chronic Obstructive Pulmonary DiseaseDocument9 pagesPrediction of Peak Oxygen Uptake From Ratings of Perceived Exertion During A Sub-Maximal Cardiopulmonary Exercise Test in Patients With Chronic Obstructive Pulmonary DiseaseJuan Pablo Casanova AnguloPas encore d'évaluation
- BCMJ 52vol9 Knee Arthroplasty PDFDocument8 pagesBCMJ 52vol9 Knee Arthroplasty PDFJuan Pablo Casanova AnguloPas encore d'évaluation
- 11gcfl2772 PDFDocument2 pages11gcfl2772 PDFJuan Pablo Casanova AnguloPas encore d'évaluation
- Effect of Electrical Stimulation On Lipolysis of Human White AdipocytesDocument5 pagesEffect of Electrical Stimulation On Lipolysis of Human White AdipocytesJuan Pablo Casanova AnguloPas encore d'évaluation
- Pubpressloenneke PDFDocument8 pagesPubpressloenneke PDFJúnior Alvacir CamargoPas encore d'évaluation
- 11gcfl2772 PDFDocument2 pages11gcfl2772 PDFJuan Pablo Casanova AnguloPas encore d'évaluation
- 10 1111@j 1600-0838 2012 01489 XDocument7 pages10 1111@j 1600-0838 2012 01489 XJuan Pablo Casanova AnguloPas encore d'évaluation
- 1-Ligamentos: Cervical AltoDocument3 pages1-Ligamentos: Cervical AltoJuan Pablo Casanova AnguloPas encore d'évaluation
- Full TextDocument7 pagesFull TextJuan Pablo Casanova AnguloPas encore d'évaluation
- Mulligan Concept Conference Abstract BookDocument89 pagesMulligan Concept Conference Abstract BookMichel BakkerPas encore d'évaluation
- El Sistema GRADE: Un Cambio en La Forma de Evaluar La Calidad de La Evidencia y La Fuerza de RecomendacionesDocument6 pagesEl Sistema GRADE: Un Cambio en La Forma de Evaluar La Calidad de La Evidencia y La Fuerza de RecomendacionesJuan Pablo Casanova AnguloPas encore d'évaluation
- Classification PDFDocument55 pagesClassification PDFJuan Pablo Casanova AnguloPas encore d'évaluation
- Cull Inane 2013Document18 pagesCull Inane 2013Juan Pablo Casanova AnguloPas encore d'évaluation
- 11 GCFL 2772Document2 pages11 GCFL 2772Juan Pablo Casanova AnguloPas encore d'évaluation
- Abnormal Heart Rate Recovery and Chronotropic Incompetence On Exercise in Chronic Obstructive Pulmonary DiseaseDocument11 pagesAbnormal Heart Rate Recovery and Chronotropic Incompetence On Exercise in Chronic Obstructive Pulmonary DiseaseJuan Pablo Casanova AnguloPas encore d'évaluation
- Cervical Spine InjuriesDocument51 pagesCervical Spine InjuriesJuan Pablo Casanova AnguloPas encore d'évaluation
- 10 1111@j 1600-0838 2012 01489 XDocument7 pages10 1111@j 1600-0838 2012 01489 XJuan Pablo Casanova AnguloPas encore d'évaluation
- 10.1007@s00421 016 3447 2Document9 pages10.1007@s00421 016 3447 2Juan Pablo Casanova AnguloPas encore d'évaluation
- 4 Methodological Considerations For Blood Flow Restricted Resistance Exercise 2012 - 1 - 14-22 PDFDocument9 pages4 Methodological Considerations For Blood Flow Restricted Resistance Exercise 2012 - 1 - 14-22 PDFJuan Pablo Casanova AnguloPas encore d'évaluation
- Biophysj00315 0078 PDFDocument17 pagesBiophysj00315 0078 PDFJuan Pablo Casanova AnguloPas encore d'évaluation
- LIFTING PERFORMANCE OF THE SY215C EXCAVATORDocument4 pagesLIFTING PERFORMANCE OF THE SY215C EXCAVATORAkhmad SebehPas encore d'évaluation
- Mid Drive Vs HubDocument15 pagesMid Drive Vs HubRivan PamungkasPas encore d'évaluation
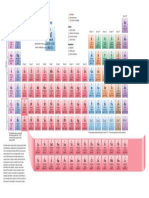
- Periodic TableDocument1 pagePeriodic TableChemist MookaPas encore d'évaluation
- The Use and Misuse of SEMDocument30 pagesThe Use and Misuse of SEMPPDTBM renPas encore d'évaluation
- Projectile LoomDocument23 pagesProjectile Loommehedi111560% (5)
- Two Sigma - LeetCodeDocument2 pagesTwo Sigma - LeetCodePeeyushPas encore d'évaluation
- 5437 1Document190 pages5437 1Khateeb RehmanPas encore d'évaluation
- Record results of toy soldier experiment times with different massesDocument42 pagesRecord results of toy soldier experiment times with different massesTeoh Han Jie100% (1)
- Notes 3 - Consistent Deformation DerivationDocument3 pagesNotes 3 - Consistent Deformation DerivationAdi DeckPas encore d'évaluation
- Pritchett Clock Repair Shop Breakeven Analysis ExcelDocument138 pagesPritchett Clock Repair Shop Breakeven Analysis ExcelMohd Yousuf MasoodPas encore d'évaluation
- Add Nordic Semiconductor DFU To SDK Example: Bluetooth Low EnergyDocument32 pagesAdd Nordic Semiconductor DFU To SDK Example: Bluetooth Low EnergyDaniel Ernesto EspitiaPas encore d'évaluation
- Raman BandsDocument2 pagesRaman Bandspreyas1Pas encore d'évaluation
- Introduction To Music Theory: Inversions of ChordsDocument3 pagesIntroduction To Music Theory: Inversions of Chordsnaveenmanuel8879Pas encore d'évaluation
- Battery ModelingDocument6 pagesBattery ModelingmusabnajeebPas encore d'évaluation
- Flight Planning For ATTDocument106 pagesFlight Planning For ATTTienek Lee100% (1)
- Measuring AssignmentDocument3 pagesMeasuring AssignmentArnab BhattacharyaPas encore d'évaluation
- Laura Hasley Statistics-Chi-Squared Goodness of Fit Test Lesson PlanDocument11 pagesLaura Hasley Statistics-Chi-Squared Goodness of Fit Test Lesson Planapi-242213383Pas encore d'évaluation
- Tensile FinalDocument43 pagesTensile Finalnamrataavyas75% (4)
- Well CompletionDocument26 pagesWell Completionnitesh kumarPas encore d'évaluation
- TVS Apache RTR 180 Service ManualDocument25 pagesTVS Apache RTR 180 Service ManualSandino JosePas encore d'évaluation
- Erection Manual Hydro-1Document63 pagesErection Manual Hydro-1rajfab100% (1)
- Tool Geometry and Tool LifeDocument29 pagesTool Geometry and Tool LifeSudeepHandikherkarPas encore d'évaluation
- Fire ZoneDocument8 pagesFire ZoneKannan NPas encore d'évaluation
- Blockchain Technology For Cloud Storage - A Systematic Literature ReviewDocument33 pagesBlockchain Technology For Cloud Storage - A Systematic Literature ReviewNgocPas encore d'évaluation
- Excel ShortcutsDocument21 pagesExcel Shortcutsrushishinde9797Pas encore d'évaluation
- HW 11Document7 pagesHW 11Devendraa MuniandyPas encore d'évaluation
- A e Regulator GuideDocument1 pageA e Regulator Guidenasser4858Pas encore d'évaluation
- Quad Encoder Velocity Accel with CRIOLabVIEW FPGADocument5 pagesQuad Encoder Velocity Accel with CRIOLabVIEW FPGAChâu Tinh TrìPas encore d'évaluation
- AAL1 and Segmentation and Reassembly LayerDocument18 pagesAAL1 and Segmentation and Reassembly Layeroureducation.inPas encore d'évaluation
- Product Guide (English 140702)Document11 pagesProduct Guide (English 140702)Dineshkumar MahedranPas encore d'évaluation