Vous aimerez peut-être aussi
- RX Dentist Itrs Final RestorationDocument1 pageRX Dentist Itrs Final RestorationdamingeniusPas encore d'évaluation
- Ddslab RX RemDocument1 pageDdslab RX Remdrmohamad drmohamadPas encore d'évaluation
- RX Dentist RemovableDocument2 pagesRX Dentist RemovabledamingeniusPas encore d'évaluation
- Catalogo Minarik PDFDocument96 pagesCatalogo Minarik PDFCarlos Vazquez Vazquez67% (3)
- Laboratory Procedure Prescription: RetainersDocument1 pageLaboratory Procedure Prescription: Retainersdrmohamad drmohamadPas encore d'évaluation
- Please Attached For Con: Project Name Location: ....... Floor Carpark Area: Date: Daswin Office Tower ProjectDocument4 pagesPlease Attached For Con: Project Name Location: ....... Floor Carpark Area: Date: Daswin Office Tower ProjectWahyu Rohmad DiantoPas encore d'évaluation
- Casting 2324Document85 pagesCasting 2324saurabhmagar333Pas encore d'évaluation
- Structural ModelingDocument21 pagesStructural ModelingWilbert ReuyanPas encore d'évaluation
- Sewing Silver SparkDocument15 pagesSewing Silver SparkRahul SasidharanPas encore d'évaluation
- 2021 Pisa 2 Cut Sheet - UnilockDocument3 pages2021 Pisa 2 Cut Sheet - UnilockjeamilPas encore d'évaluation
- Catalog KennametalDocument749 pagesCatalog KennametalTrí PhạmPas encore d'évaluation
- Guide To CBN & PCD Turning Inserts: Section OrganizationDocument66 pagesGuide To CBN & PCD Turning Inserts: Section OrganizationKasia MazurPas encore d'évaluation
- GKM Series (Global Miniature Safety Key Interlock Switch) : FeaturesDocument100 pagesGKM Series (Global Miniature Safety Key Interlock Switch) : FeaturesyonesPas encore d'évaluation
- Okadia - Knowledge Brief Pm#11Document6 pagesOkadia - Knowledge Brief Pm#11Maurel ADJEIPas encore d'évaluation
- Digital SAT Prep in CaliforniaDocument18 pagesDigital SAT Prep in Californiasarika523Pas encore d'évaluation
- Checklist of Enclose-Rev00Document1 pageChecklist of Enclose-Rev00muth sokvisalPas encore d'évaluation
- BETE_N-metricDocument1 pageBETE_N-metricDenaibeliPas encore d'évaluation
- Feeder Pillar 03 (FGB - 01-And Fgb-02)Document4 pagesFeeder Pillar 03 (FGB - 01-And Fgb-02)Natasha de SilvaPas encore d'évaluation
- 17052023-Layout DB Wing 01 RDocument78 pages17052023-Layout DB Wing 01 RSann SeyhaPas encore d'évaluation
- SMT Process MapDocument1 pageSMT Process Map210151 JOSE MANUEL RAMIREZ PINEDAPas encore d'évaluation
- b5-150 Screens EngDocument7 pagesb5-150 Screens Engjahangir_alam44_6764Pas encore d'évaluation
- Prototype PCB - Online PCB Quote - Full Feature Custom PCB Prototype Service at Low Cost - PCBWayDocument2 pagesPrototype PCB - Online PCB Quote - Full Feature Custom PCB Prototype Service at Low Cost - PCBWaygabriel100matosPas encore d'évaluation
- Introduction To NovaFlowSolidDocument13 pagesIntroduction To NovaFlowSolidNeven GvozdAnovićPas encore d'évaluation
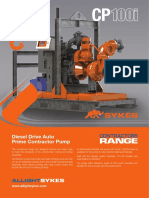
- AS SpecSheet - CP100iDocument2 pagesAS SpecSheet - CP100iFrank RodriguezPas encore d'évaluation
- Design of Beams: CE 382 Reinforced Concrete FundamentalsDocument8 pagesDesign of Beams: CE 382 Reinforced Concrete FundamentalsElif UlusoyPas encore d'évaluation
- GulfJobPaper 9 OctDocument3 pagesGulfJobPaper 9 OctJKHSDJFURHPas encore d'évaluation
- Diesel Drive Auto Prime XTRA High Head PumpDocument2 pagesDiesel Drive Auto Prime XTRA High Head Pumpekho_febryPas encore d'évaluation
- Specification For Instrument Cable: Pecification For Nstrument AbleDocument18 pagesSpecification For Instrument Cable: Pecification For Nstrument Ableamini_mohiPas encore d'évaluation
- Amega Line Data Sheet FinalDocument2 pagesAmega Line Data Sheet Finalapi-19852580Pas encore d'évaluation
- PD-F 03 .Engineering Change Note - Internal & Sup. InitiationDocument2 pagesPD-F 03 .Engineering Change Note - Internal & Sup. InitiationHarjeet SinghPas encore d'évaluation
- Guide To Turning Inserts: CN RTGDocument180 pagesGuide To Turning Inserts: CN RTGIwan Setiawan Part IIPas encore d'évaluation
- 2019 Version ComparisonDocument1 page2019 Version Comparisonsathiya priyaPas encore d'évaluation
- Nachi Robot Catalog 1Document30 pagesNachi Robot Catalog 1faisalPas encore d'évaluation
- Cube Register LogDocument1 pageCube Register LogNickPas encore d'évaluation
- Biobase Microscope BrochureDocument3 pagesBiobase Microscope BrochureJim DonairePas encore d'évaluation
- Catalog c009b B CBN PCD InsertsDocument82 pagesCatalog c009b B CBN PCD Insertsnguyễn khắc namPas encore d'évaluation
- Jay Bhart Maruti Ltd. Vithalapur, Gujarat: (Performance Evaluation)Document15 pagesJay Bhart Maruti Ltd. Vithalapur, Gujarat: (Performance Evaluation)Sharwan KumarPas encore d'évaluation
- Premier Line Data Sheet FinalDocument2 pagesPremier Line Data Sheet Finalapi-19852580Pas encore d'évaluation
- MBV - Products - List V-Belt VNDocument1 pageMBV - Products - List V-Belt VNSteven PhamPas encore d'évaluation
- Process Technology For recoveredCarbonBlack - enDocument4 pagesProcess Technology For recoveredCarbonBlack - enVivek MorePas encore d'évaluation
- Intntl Line Data Sheet FinalDocument2 pagesIntntl Line Data Sheet Finalapi-19852580Pas encore d'évaluation
- Viscosity Sample Information Sheet PDFDocument1 pageViscosity Sample Information Sheet PDFsivhongPas encore d'évaluation
- Viscosity Sample Information SheetDocument1 pageViscosity Sample Information SheetPim NavaPas encore d'évaluation
- Group Catalog Sprocket PDFDocument17 pagesGroup Catalog Sprocket PDFFaisal Rahman ArifPas encore d'évaluation
- Beijing E Solvent Technologies Corp 400.000 of Oil-Sand Separator Device Data Sheet of AgitatorDocument4 pagesBeijing E Solvent Technologies Corp 400.000 of Oil-Sand Separator Device Data Sheet of AgitatoridilfitriPas encore d'évaluation
- Feeder Pillar 01 (Aopv-01 and Opv - 01)Document4 pagesFeeder Pillar 01 (Aopv-01 and Opv - 01)Natasha de SilvaPas encore d'évaluation
- Quality Assurance: Revisions ClientDocument1 pageQuality Assurance: Revisions ClientDhairya ShahPas encore d'évaluation
- Master Data: Unit Test Scenario Id: NRC - Ut - Co - Master Data - 001 - 1.0Document4 pagesMaster Data: Unit Test Scenario Id: NRC - Ut - Co - Master Data - 001 - 1.0Haytham DawoudPas encore d'évaluation
- Building 90° Corners - Ts298Document2 pagesBuilding 90° Corners - Ts298ZebPas encore d'évaluation
- Production Study Sheet: Effective Non Effective ActivitiesDocument3 pagesProduction Study Sheet: Effective Non Effective Activitieslodestar iePas encore d'évaluation
- Technology and Concepts For Sika Carbodur Structural Strengthening SystemsDocument11 pagesTechnology and Concepts For Sika Carbodur Structural Strengthening Systemsj2bstation stadinPas encore d'évaluation
- GPZ 900Document3 pagesGPZ 900capimrfloydPas encore d'évaluation
- Pin BorDocument1 pagePin Borsofiatun khoirohPas encore d'évaluation
- Mechanical AbrasivesDocument8 pagesMechanical AbrasivesVictor Javier Reyes NavarroPas encore d'évaluation
- Flexible Clay Tiles-BRDDocument30 pagesFlexible Clay Tiles-BRDjaykhor9328Pas encore d'évaluation
- Bobcat 853 BackhoesDocument6 pagesBobcat 853 Backhoeschris caseyPas encore d'évaluation
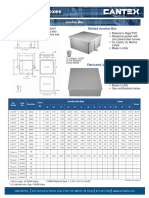
- CANTEX Junction Box Sell SheetDocument1 pageCANTEX Junction Box Sell SheetARNOLDPas encore d'évaluation
- August & September Monthly Collection, Grade 1D'EverandAugust & September Monthly Collection, Grade 1Pas encore d'évaluation
- Show Annoyance: BBC Learning English HowtoDocument4 pagesShow Annoyance: BBC Learning English HowtodamingeniusPas encore d'évaluation
- 1 - How To 080213 Positive NegativeDocument4 pages1 - How To 080213 Positive NegativeValentin CapraruPas encore d'évaluation
- Howto 071030 Accepting ApologiesDocument4 pagesHowto 071030 Accepting ApologiesAnandPas encore d'évaluation
- GL Inclusive 2740 111017Document2 pagesGL Inclusive 2740 111017damingeniusPas encore d'évaluation
- Aae Keep UpDocument2 pagesAae Keep UpdamingeniusPas encore d'évaluation
- 6min English Learning A LanguageDocument4 pages6min English Learning A LanguageAlex RaduPas encore d'évaluation
- GL Implant Removable 2285 11061717Document2 pagesGL Implant Removable 2285 11061717damingeniusPas encore d'évaluation
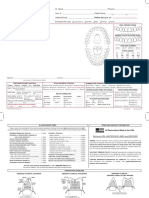
- Deliver by 5 P.M. On - : See Reverse For Working TimesDocument2 pagesDeliver by 5 P.M. On - : See Reverse For Working TimesdamingeniusPas encore d'évaluation
- RX Dentist Inclusive Tissue Contouring SolutionDocument2 pagesRX Dentist Inclusive Tissue Contouring SolutiondamingeniusPas encore d'évaluation
- RX Dentist CanadaDocument2 pagesRX Dentist CanadadamingeniusPas encore d'évaluation
- RX Dentist Fixed PDFDocument2 pagesRX Dentist Fixed PDFdamingeniusPas encore d'évaluation
- RX Dentist Bruxzir Implant ProsthesisDocument2 pagesRX Dentist Bruxzir Implant ProsthesisdamingeniusPas encore d'évaluation
- Java Code ConventionsDocument24 pagesJava Code ConventionsLeeLiPas encore d'évaluation
- Java Code ConventionsDocument24 pagesJava Code ConventionsLeeLiPas encore d'évaluation
- Complications Following Dental Extractions in A Mobile Dental ClinicDocument4 pagesComplications Following Dental Extractions in A Mobile Dental ClinicdamingeniusPas encore d'évaluation
- Java Code ConventionsDocument24 pagesJava Code ConventionsLeeLiPas encore d'évaluation
- Biologic Width and Crown Lengthening Case StudiesDocument7 pagesBiologic Width and Crown Lengthening Case StudiesSusi LpjPas encore d'évaluation
- All-Ceramic or Metal-Ceramic Tooth-Supported Fixed Dental Prostheses (FDPS) A Systematic Review of The Survival and Complication Rates Part I Single CrownsDocument21 pagesAll-Ceramic or Metal-Ceramic Tooth-Supported Fixed Dental Prostheses (FDPS) A Systematic Review of The Survival and Complication Rates Part I Single CrownsmahmoudPas encore d'évaluation
- Provisional Restorations in Fixed Prosthodontics: Charles J. Goodacre, DDS, MSDDocument36 pagesProvisional Restorations in Fixed Prosthodontics: Charles J. Goodacre, DDS, MSDBharathi GudapatiPas encore d'évaluation
- Prostho McqsDocument16 pagesProstho Mcqs_RedX_Pas encore d'évaluation
- All-Ceramic Silica/glass-Based Crowns - Clinical Protocols: B. MizrahiDocument6 pagesAll-Ceramic Silica/glass-Based Crowns - Clinical Protocols: B. Mizrahijesuscomingsoon2005_100% (1)
- Restorative Space and Occlusal Evaluation RPDDocument48 pagesRestorative Space and Occlusal Evaluation RPDKulashekar ReddyPas encore d'évaluation
- Connector Design PrinciplesDocument24 pagesConnector Design PrinciplesVikas Aggarwal100% (1)
- Zirconnia Knife Edge PDFDocument6 pagesZirconnia Knife Edge PDFMuaiyed Buzayan AkremyPas encore d'évaluation
- Non Preparation VeneersDocument24 pagesNon Preparation VeneersastinejenniferPas encore d'évaluation
- Ceramic Laminate VeneersDocument23 pagesCeramic Laminate VeneersGerard Andrei Arlovski100% (2)
- Various Attachments Used in Prosthodontics-A Review: November 2018Document5 pagesVarious Attachments Used in Prosthodontics-A Review: November 2018harshita parasharPas encore d'évaluation
- Dha 2015 PDFDocument99 pagesDha 2015 PDFSingh Vidhi100% (4)
- History of DentistryDocument38 pagesHistory of DentistrydrpretheeptPas encore d'évaluation
- Dental Veneers - Template Dentaire - PDF DENTAL VENEERSDocument7 pagesDental Veneers - Template Dentaire - PDF DENTAL VENEERSPicincu Irina GeorgianaPas encore d'évaluation
- Dental Restorative Digital Workflow: Digital Smile Design From Aesthetic To Function PDFDocument12 pagesDental Restorative Digital Workflow: Digital Smile Design From Aesthetic To Function PDFCamilo GuerreroPas encore d'évaluation
- Adhesive BridgesDocument9 pagesAdhesive BridgesShilpa ShrivastavaPas encore d'évaluation
- Emax PDFDocument68 pagesEmax PDFseby996arPas encore d'évaluation
- Types of finish lines in tooth preparationDocument6 pagesTypes of finish lines in tooth preparationSahana RangarajanPas encore d'évaluation
- OverdentureDocument76 pagesOverdentureRaj Sha80% (5)
- A New Classification System For All-Ceramic and Ceramic-Like Restorative Materials. 2015 - Gracis - IJPDocument11 pagesA New Classification System For All-Ceramic and Ceramic-Like Restorative Materials. 2015 - Gracis - IJPPaul AlvarezPas encore d'évaluation
- Color Atlas of Dental Implant Surgery - Saunders 3rd Edition (April 13, 2010) PDFDocument479 pagesColor Atlas of Dental Implant Surgery - Saunders 3rd Edition (April 13, 2010) PDFDumitru Nuca100% (6)
- FTHHHDocument17 pagesFTHHHSaad khanPas encore d'évaluation
- Ipd 2015 NewsDocument16 pagesIpd 2015 Newsapi-252208131100% (1)
- Surveyor & Parts of Surveyor in RDocument101 pagesSurveyor & Parts of Surveyor in RBharanijaPas encore d'évaluation
- Andre V. Ritter - Sturdevant's Art and Science of Operative Dentistry-Mosby (2018) - 149-182-DikonversiDocument55 pagesAndre V. Ritter - Sturdevant's Art and Science of Operative Dentistry-Mosby (2018) - 149-182-DikonversiMuhammad AlpinPas encore d'évaluation
- Deep Margin ElevationDocument11 pagesDeep Margin Elevationjarodzee100% (4)
- Metal Ceramic RestorationDocument48 pagesMetal Ceramic RestorationZy Hoe75% (4)
- HTTP WWW - Iusd.iupui - Edu IndexDocument20 pagesHTTP WWW - Iusd.iupui - Edu IndexReema MazenPas encore d'évaluation
- Universal Dental Gold AlloysDocument6 pagesUniversal Dental Gold Alloysryu100Pas encore d'évaluation
- Recent Advances in Provisional RestorationsDocument6 pagesRecent Advances in Provisional RestorationsAngelia PratiwiPas encore d'évaluation