Vous aimerez peut-être aussi
- Katherine J Gold Sheila M Marcus: Table 1Document4 pagesKatherine J Gold Sheila M Marcus: Table 1angelie21Pas encore d'évaluation
- Fitzpatricks Dermatology in General Medicine 8ed 1Document10 pagesFitzpatricks Dermatology in General Medicine 8ed 1ANTINPas encore d'évaluation
- Acute Kidney InjuryDocument49 pagesAcute Kidney InjuryfikasywPas encore d'évaluation
- Optimal Birth Spacing: What Can We Measure and What Do We Want To Know?Document3 pagesOptimal Birth Spacing: What Can We Measure and What Do We Want To Know?rizmahPas encore d'évaluation
- HHS Public AccessDocument16 pagesHHS Public AccessMahlina Nur LailiPas encore d'évaluation
- Efectele Pe Termen Lung Ale Alaptatului OMSDocument74 pagesEfectele Pe Termen Lung Ale Alaptatului OMSbobocraiPas encore d'évaluation
- Laborinduction: Areviewof Currentmethods: Mildred M. RamirezDocument11 pagesLaborinduction: Areviewof Currentmethods: Mildred M. RamirezRolando DiazPas encore d'évaluation
- The Natural History of The Normal First Stage Of.6 PDFDocument6 pagesThe Natural History of The Normal First Stage Of.6 PDFreioctabianoPas encore d'évaluation
- Birth Plans: Birth Preferences or Labor Manifesto: Imedpub JournalsDocument4 pagesBirth Plans: Birth Preferences or Labor Manifesto: Imedpub JournalsDesde Chile Hasta AlaskaPas encore d'évaluation
- ACOG Committee Opinion #697 Planned Home BirthDocument6 pagesACOG Committee Opinion #697 Planned Home Birthjoselinrivero92Pas encore d'évaluation
- Articulo Peruano PDFDocument10 pagesArticulo Peruano PDFStephanyChavezFeriaPas encore d'évaluation
- Primary and Secondary Infertility NotesDocument17 pagesPrimary and Secondary Infertility NotesMeangafo GraciaPas encore d'évaluation
- Care in Pregnancies Subsequent To Stillbirthor Perinatal DeatDocument12 pagesCare in Pregnancies Subsequent To Stillbirthor Perinatal DeatgalalPas encore d'évaluation
- D'Souza-2019-Maternal Body Mass Index and PregDocument17 pagesD'Souza-2019-Maternal Body Mass Index and PregMARIATUL QIFTIYAHPas encore d'évaluation
- Effect of Placenta Previa On Fetal Growth: ObstetricsDocument5 pagesEffect of Placenta Previa On Fetal Growth: ObstetricsAnonymous 4OpLzzt6Pas encore d'évaluation
- Women 'S Experiences of Planning A Vaginal Birth After Caesarean in Different Models of Maternity Care in AustraliaDocument15 pagesWomen 'S Experiences of Planning A Vaginal Birth After Caesarean in Different Models of Maternity Care in AustraliasryPas encore d'évaluation
- Nihms666259Document15 pagesNihms666259miss betawiPas encore d'évaluation
- Bhattacharya Bhattacharya 2009 Effect of Miscarriage On Future PregnanciesDocument4 pagesBhattacharya Bhattacharya 2009 Effect of Miscarriage On Future PregnanciesPutu Gede WidyatamaPas encore d'évaluation
- 2018 Article 414Document18 pages2018 Article 414Haribabu ArumugamPas encore d'évaluation
- Postpartum Lit Review NealeDocument9 pagesPostpartum Lit Review Nealeapi-726948535Pas encore d'évaluation
- Women's Health Care Physicians: Member Login Join Pay Dues Follow UsDocument24 pagesWomen's Health Care Physicians: Member Login Join Pay Dues Follow UsNazif Aiman IsmailPas encore d'évaluation
- Nihms 906378Document13 pagesNihms 906378yuliana khairiPas encore d'évaluation
- 332 Short Interpregnancy Interval: Definition/Cut-off ValueDocument4 pages332 Short Interpregnancy Interval: Definition/Cut-off ValueRonald David Suca SaavedraPas encore d'évaluation
- Recurrent Implantation Failure-Update Overview OnDocument19 pagesRecurrent Implantation Failure-Update Overview Onn2763288100% (1)
- Journal Reading: Influence of Interpregnancy Interval On Uterine RuptureDocument9 pagesJournal Reading: Influence of Interpregnancy Interval On Uterine RuptureIlham ErtandriPas encore d'évaluation
- Duong2012sexuality Contraception Breastfeeding PDFDocument8 pagesDuong2012sexuality Contraception Breastfeeding PDFMelonsmasherPas encore d'évaluation
- Debate GUIDE PDFDocument8 pagesDebate GUIDE PDFBlesse PateñoPas encore d'évaluation
- Comparison of Adequacy of Birth Weight For Gestational Age According To Different Intrauterine Growth CurvesDocument6 pagesComparison of Adequacy of Birth Weight For Gestational Age According To Different Intrauterine Growth CurvesSilvie WidyaPas encore d'évaluation
- Running Head: HEALTH POLICY PAPER 1Document10 pagesRunning Head: HEALTH POLICY PAPER 1api-283540594Pas encore d'évaluation
- Tinjauan Pustaka Persalinan NormalDocument31 pagesTinjauan Pustaka Persalinan NormalNurul Fathia Shafira AmiantiPas encore d'évaluation
- 2022 The Diagnosis and Management of Suspected Fetal Growth Restriction and Evidence Based ApproachDocument13 pages2022 The Diagnosis and Management of Suspected Fetal Growth Restriction and Evidence Based ApproachHillary AchachPas encore d'évaluation
- Home BirthDocument33 pagesHome BirthMarlon Royo100% (2)
- Finocchario-Kessler Miscarriage 2018Document5 pagesFinocchario-Kessler Miscarriage 2018Ari StaggsPas encore d'évaluation
- To Ignore or Not To Ignore Placental Calcifications On Prenatal Ultrasound: A Systematic Review and Meta-AnalysisDocument22 pagesTo Ignore or Not To Ignore Placental Calcifications On Prenatal Ultrasound: A Systematic Review and Meta-AnalysisMaulida HalimahPas encore d'évaluation
- Ijogr 6 4 466 468Document3 pagesIjogr 6 4 466 468RachnaPas encore d'évaluation
- Tocolysis For Inhibiting Preterm Birth in Extremely Preterm Birth, Multiple Gestations and in Growth-Restricted Fetuses A Systematic Review and Meta-AnalysisDocument12 pagesTocolysis For Inhibiting Preterm Birth in Extremely Preterm Birth, Multiple Gestations and in Growth-Restricted Fetuses A Systematic Review and Meta-Analysisjojhan.andres02Pas encore d'évaluation
- Marital InfertilityDocument4 pagesMarital InfertilityasclepiuspdfsPas encore d'évaluation
- Antenatal Dexamethasone For Early Preterm Birth in Low-Resource CountriesDocument12 pagesAntenatal Dexamethasone For Early Preterm Birth in Low-Resource CountriesMemento MoriPas encore d'évaluation
- To Vbac or Not To Vbac: PerspectiveDocument3 pagesTo Vbac or Not To Vbac: Perspectiveharani roimaPas encore d'évaluation
- 26 Device Improves Swallowing in Newborns: CommentDocument33 pages26 Device Improves Swallowing in Newborns: CommentWahyuni M. Ali MrePas encore d'évaluation
- Pi Is 0002937810000815 JournallDocument12 pagesPi Is 0002937810000815 JournallRaisa AriesthaPas encore d'évaluation
- FGWH 03 828052Document5 pagesFGWH 03 828052fortunat.mutelesiPas encore d'évaluation
- The Role of Labor Induction in Modern ObstetricsDocument7 pagesThe Role of Labor Induction in Modern ObstetricsKevin Stanley HalimPas encore d'évaluation
- BJOG - 2022 - Tessema - The Role of Intervening Pregnancy Loss in The Association Between Interpregnancy Interval andDocument9 pagesBJOG - 2022 - Tessema - The Role of Intervening Pregnancy Loss in The Association Between Interpregnancy Interval andAnonymous l6Q1ROq2Pas encore d'évaluation
- The Effect of Ramadan Fasting During Pregnancy On Perinatal Outcomes: A Systematic Review and Meta-AnalysisDocument11 pagesThe Effect of Ramadan Fasting During Pregnancy On Perinatal Outcomes: A Systematic Review and Meta-AnalysisUlfahPas encore d'évaluation
- Hubungn Miom Dengan IUGRDocument14 pagesHubungn Miom Dengan IUGRRizqon Yasir KoeswondoPas encore d'évaluation
- 10 1016@j Ajog 2019 01 206 PDFDocument8 pages10 1016@j Ajog 2019 01 206 PDFYusvita WaliaPas encore d'évaluation
- 10 1016@j Ajog 2019 01 206Document8 pages10 1016@j Ajog 2019 01 206Yusvita WaliaPas encore d'évaluation
- Correspondence: Breastfeeding in The 21st CenturyDocument2 pagesCorrespondence: Breastfeeding in The 21st CenturyGladys Barzola CerrónPas encore d'évaluation
- ÓbitoDocument111 pagesÓbitoDamián López RangelPas encore d'évaluation
- Safe Prevention of The Primary Cesarean Delivery - ACOGDocument16 pagesSafe Prevention of The Primary Cesarean Delivery - ACOGAryaPas encore d'évaluation
- Wiklund2012 (Indication)Document8 pagesWiklund2012 (Indication)Noah Borketey-laPas encore d'évaluation
- Preconception Care To Improve Pregnancy Outcomes: The ScienceDocument8 pagesPreconception Care To Improve Pregnancy Outcomes: The SciencekofiPas encore d'évaluation
- Post Natal CareDocument17 pagesPost Natal CareJuan Carlos AuquiPas encore d'évaluation
- Labor Induction: Citations VerifyDocument8 pagesLabor Induction: Citations VerifyjiniabrahamPas encore d'évaluation
- Spin Doctoring The ResearchDocument6 pagesSpin Doctoring The ResearchszopfaszPas encore d'évaluation
- Mental HealthDocument7 pagesMental HealthMirjana14Pas encore d'évaluation
- Low-Risk Planned Caesarean Versus Planned Vaginal Delivery at Term: Early and Late Infantile OutcomesDocument11 pagesLow-Risk Planned Caesarean Versus Planned Vaginal Delivery at Term: Early and Late Infantile OutcomesEduarda QuartinPas encore d'évaluation
- Research Paper On Pregnancy and ChildbirthDocument8 pagesResearch Paper On Pregnancy and Childbirthnywxluvkg100% (1)
- Induced Abortion and Risks That May Impact AdolescentsDocument29 pagesInduced Abortion and Risks That May Impact AdolescentsMichael RezaPas encore d'évaluation
- Low Birth Weight Literature ReviewDocument5 pagesLow Birth Weight Literature Reviewojfhsiukg100% (1)
- Diminished Ovarian Reserve and Assisted Reproductive Technologies: Current Research and Clinical ManagementD'EverandDiminished Ovarian Reserve and Assisted Reproductive Technologies: Current Research and Clinical ManagementOrhan BukulmezPas encore d'évaluation
- Obgm Feb2018 Vol.30 No.2 PDFDocument55 pagesObgm Feb2018 Vol.30 No.2 PDFlcmurilloPas encore d'évaluation
- Everyday Contraception ConsiderationsDocument15 pagesEveryday Contraception ConsiderationslcmurilloPas encore d'évaluation
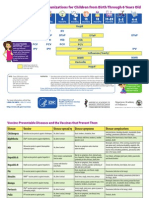
- Parent Ver SCH 0 6yrsDocument2 pagesParent Ver SCH 0 6yrslcmurilloPas encore d'évaluation
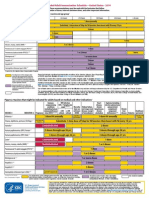
- Catchup Schedule BWDocument4 pagesCatchup Schedule BWlcmurilloPas encore d'évaluation
- Adult Schedule 11x17Document2 pagesAdult Schedule 11x17lcmurilloPas encore d'évaluation
- Adult ScheduleDocument3 pagesAdult SchedulelcmurilloPas encore d'évaluation
- Adult Combined ScheduleDocument5 pagesAdult Combined SchedulelcmurilloPas encore d'évaluation
- BSS 2018Document24 pagesBSS 2018gumoha01Pas encore d'évaluation
- Reading Sub-Test - Question Paper: Part A: Instructions To CandidatesDocument8 pagesReading Sub-Test - Question Paper: Part A: Instructions To CandidatesAditi ParmarPas encore d'évaluation
- Department of MEDICINE-1Document16 pagesDepartment of MEDICINE-1Ajay BangPas encore d'évaluation
- BORLAND D. M., Digestive Drugs (Bl6)Document51 pagesBORLAND D. M., Digestive Drugs (Bl6)ruling_geminiPas encore d'évaluation
- Ectopic Pregnancy Nursing Care PlansDocument27 pagesEctopic Pregnancy Nursing Care Plansviper7967880% (20)
- Cumulative Trauma DisordersDocument70 pagesCumulative Trauma DisordersBishal BistaPas encore d'évaluation
- Pearls ToxocologicDocument3 pagesPearls ToxocologichsbacongaPas encore d'évaluation
- Diplopia: Diagnosis and Management: Author: Saurabh JainDocument3 pagesDiplopia: Diagnosis and Management: Author: Saurabh Jainlia indria watiPas encore d'évaluation
- Chapter - 2 Microorganisms (Continuation)Document2 pagesChapter - 2 Microorganisms (Continuation)ARSHAD JAMILPas encore d'évaluation
- Eye and Ears AssessmentDocument17 pagesEye and Ears AssessmentPrincess AñabezaPas encore d'évaluation
- 33rd IACDE National Conference 2018 - VijayawadaDocument5 pages33rd IACDE National Conference 2018 - VijayawadaHari PriyaPas encore d'évaluation
- CBD Spinal Infection: by Neoh Zhong NingDocument26 pagesCBD Spinal Infection: by Neoh Zhong NingJoni NeohPas encore d'évaluation
- Walking: The 'Wonder Drug': VocabularyDocument3 pagesWalking: The 'Wonder Drug': VocabularyLiveLaugh LovePas encore d'évaluation
- Ebook John Murtaghs General Practice Companion Handbook PDF Full Chapter PDFDocument67 pagesEbook John Murtaghs General Practice Companion Handbook PDF Full Chapter PDFroberto.duncan209100% (27)
- Radiographic Aids in The Diagnosis of Periodontal Diseases: Presented By: DR: Abdullah AliDocument27 pagesRadiographic Aids in The Diagnosis of Periodontal Diseases: Presented By: DR: Abdullah AliMugahed Abdo Al-gahdariPas encore d'évaluation
- Functional Gastrointestinal Disorders History Pathophysiology Clinical Features and Rome IVDocument20 pagesFunctional Gastrointestinal Disorders History Pathophysiology Clinical Features and Rome IVwenyinriantoPas encore d'évaluation
- I. General Physical AssessmentDocument5 pagesI. General Physical AssessmentmnlstrPas encore d'évaluation
- (S-W5-Sun-Gen.S) (By Dr. Emad) Gall Bladder 1Document28 pages(S-W5-Sun-Gen.S) (By Dr. Emad) Gall Bladder 1Haider Nadhem AL-rubaiPas encore d'évaluation
- 2 Bachelor of Optometry (B Optom) 1Document7 pages2 Bachelor of Optometry (B Optom) 1Rehana ThapaPas encore d'évaluation
- Diarrhoea Patient InformationDocument3 pagesDiarrhoea Patient InformationIgor DemićPas encore d'évaluation
- NeprolithotomyDocument3 pagesNeprolithotomyjesse caballeroPas encore d'évaluation
- ISMP Voluume 15 No 10 Oct 2017-NurseAdviseERR201710Document4 pagesISMP Voluume 15 No 10 Oct 2017-NurseAdviseERR201710uss uusPas encore d'évaluation
- Chemical Toxicity Summit Day 6Document5 pagesChemical Toxicity Summit Day 6Paul Ioan PopescuPas encore d'évaluation
- Case Analysis PediatricsDocument31 pagesCase Analysis PediatricsLYNDLY AGAGEOPas encore d'évaluation
- Existing Restoration - Clinical Status: Secondary Caries Marginal Integrity Biomechanical FormDocument47 pagesExisting Restoration - Clinical Status: Secondary Caries Marginal Integrity Biomechanical FormDaniel WangPas encore d'évaluation
- 5 4 3 2 1 Grounding Techniqueqspae PDFDocument2 pages5 4 3 2 1 Grounding Techniqueqspae PDFsheetcherry57Pas encore d'évaluation
- Alkaloids Physiological EffectsDocument25 pagesAlkaloids Physiological EffectsGiang Lam100% (1)
- It Just Makes Sense 2012Document25 pagesIt Just Makes Sense 2012Emf RefugeePas encore d'évaluation