Vous aimerez peut-être aussi
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- COPD - Drug FormularyDocument32 pagesCOPD - Drug FormularyCharles BayogPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- ENT-5.1-Cosmetic and Reconstructive SurgeryDocument7 pagesENT-5.1-Cosmetic and Reconstructive SurgeryCharles BayogPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- PEDIATRICS CaseDocument17 pagesPEDIATRICS CaseCharles BayogPas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Pediatric ImmunologyDocument12 pagesPediatric ImmunologyCharles BayogPas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Treatment & Prognosis of Ewing Sarcoma (Charles)Document5 pagesTreatment & Prognosis of Ewing Sarcoma (Charles)Charles BayogPas encore d'évaluation
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- PCOL - Chapter 11 - Anti Hypertensive AgentsDocument3 pagesPCOL - Chapter 11 - Anti Hypertensive AgentsCharles BayogPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
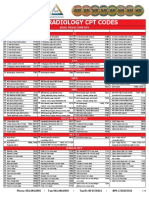
- 2019 Radiology CPT Codes: CT Bone DensitometryDocument2 pages2019 Radiology CPT Codes: CT Bone DensitometryDownsyndrome CyborgPas encore d'évaluation
- Gardner 1948Document19 pagesGardner 1948mitroisergiuPas encore d'évaluation
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- It Divides The Body Into Unequal Left and Right Plane.: Anatomical Planes, Positions and MarksDocument3 pagesIt Divides The Body Into Unequal Left and Right Plane.: Anatomical Planes, Positions and MarksCrystal Jade RetuyaPas encore d'évaluation
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- 7DO Day2Document17 pages7DO Day2Harjit Singh100% (1)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Acupressure PDFDocument46 pagesAcupressure PDFArushi100% (7)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- Life Gonstead ClubDocument29 pagesLife Gonstead Clubgonsteadtruth100% (1)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- ID 7851 Стомат Англ Задачі 1540 English Sem 2Document237 pagesID 7851 Стомат Англ Задачі 1540 English Sem 2acerPas encore d'évaluation
- Mod 1.2 Musculoskeletal System UpdatedDocument26 pagesMod 1.2 Musculoskeletal System UpdatedNandhkishorePas encore d'évaluation
- Bridging Ortho NotesDocument4 pagesBridging Ortho NotesJonathan TayPas encore d'évaluation
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- For OlgaDocument16 pagesFor OlgaEscu NykuPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Regional Anatomy Question - FinalDocument8 pagesRegional Anatomy Question - FinalManju ShreePas encore d'évaluation
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- 9 Giles B3Document37 pages9 Giles B3Jem Rhod CamensePas encore d'évaluation
- Anatomy of Pelvis and Fetal SkullDocument41 pagesAnatomy of Pelvis and Fetal SkullHakimah K. Suhaimi100% (1)
- (STUART MCGILL - Core Training Evidence Translating To Better PerfoDocument15 pages(STUART MCGILL - Core Training Evidence Translating To Better PerfoSakip Hirrim100% (2)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- NSCA - Core TrainingDocument9 pagesNSCA - Core Trainingjewndwdb100% (1)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Caroline Stone. Osteopathic ApproachDocument54 pagesCaroline Stone. Osteopathic ApproachIoan Andra100% (5)
- (Ebook - Fitness) - Stretching To PerfectionDocument15 pages(Ebook - Fitness) - Stretching To PerfectionBrooken_Arrow100% (3)
- Evidence Vrunning AnalysisDocument30 pagesEvidence Vrunning Analysisjoao manoelPas encore d'évaluation
- The Prostate Is A Common Site of Carcinoma. It: Abdomen and PelvisDocument62 pagesThe Prostate Is A Common Site of Carcinoma. It: Abdomen and PelvissrisakthiPas encore d'évaluation
- Lumbar Spine ExaminationDocument6 pagesLumbar Spine ExaminationSaddam Kanaan100% (1)
- Abnormal GaitDocument17 pagesAbnormal Gaitsalman-iqbal-329Pas encore d'évaluation
- Complete Guide To Building A Massive Back! - Cut and JackedDocument7 pagesComplete Guide To Building A Massive Back! - Cut and JackedJavier SomarribaPas encore d'évaluation
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- APT+Solution+Guide+v 1Document35 pagesAPT+Solution+Guide+v 1SamPas encore d'évaluation
- The Vulva - Structure - Innervation - TeachMeAnatomyDocument3 pagesThe Vulva - Structure - Innervation - TeachMeAnatomywzt2001Pas encore d'évaluation
- Leson Plan FEMALE PELVISDocument8 pagesLeson Plan FEMALE PELVISPreeti SawantPas encore d'évaluation
- Ischiorectal Fossa Anatomy and It's Suppuration: DR - Niveditha S Dr.S.Chandak DR - Melissa P Dr.C.MahkalkarDocument18 pagesIschiorectal Fossa Anatomy and It's Suppuration: DR - Niveditha S Dr.S.Chandak DR - Melissa P Dr.C.MahkalkarSagarRathodPas encore d'évaluation
- Malpresentations: Liji Raichel Kurian Dept of OBGDocument41 pagesMalpresentations: Liji Raichel Kurian Dept of OBGliji raichel kurian100% (1)
- Assignment 1 Skeletal SystemDocument3 pagesAssignment 1 Skeletal Systemjodi_clark_8100% (2)
- The Pelvic Floor (Pelvic Diaphragm)Document69 pagesThe Pelvic Floor (Pelvic Diaphragm)Abebe TilahunPas encore d'évaluation
- Traumatic Testicular Dislocation Associated With LDocument4 pagesTraumatic Testicular Dislocation Associated With Lcollestein christdianPas encore d'évaluation
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)