Vous aimerez peut-être aussi
- Family Nursing Care Plan Community DXDocument59 pagesFamily Nursing Care Plan Community DXSabrina Porquiado Magañan SNPas encore d'évaluation
- Family Case StudyDocument61 pagesFamily Case StudyArsenvine CabanPas encore d'évaluation
- FNCPDocument26 pagesFNCPSugar Capule - ManuelPas encore d'évaluation
- Family Nursing Process: Initial DatabaseDocument39 pagesFamily Nursing Process: Initial DatabaseMariz Joy Gonzales Guillermo100% (1)
- FNCP NewDocument29 pagesFNCP NewKhim Margarette DionisioPas encore d'évaluation
- Sample FNCP Accident HazardDocument2 pagesSample FNCP Accident HazardMichael PiducaPas encore d'évaluation
- U.S. Census Bureau:: What Is Family?Document39 pagesU.S. Census Bureau:: What Is Family?Djaryl D. Dela RiartePas encore d'évaluation
- Roquero, FNCPDocument22 pagesRoquero, FNCPGynesis Lim RoqueroPas encore d'évaluation
- Nursing Problems TypologyDocument8 pagesNursing Problems TypologyClifford Ogad0% (1)
- Sample of Case PresentationDocument43 pagesSample of Case PresentationAyaBasilio100% (1)
- Blood Pressure Measurement Is An Important Part of The Patient's Data Base. It Is Considered To BeDocument1 pageBlood Pressure Measurement Is An Important Part of The Patient's Data Base. It Is Considered To BeMir MirPas encore d'évaluation
- Family Nursing Care PlanDocument50 pagesFamily Nursing Care PlanE.R.OPas encore d'évaluation
- Family Health AssessmentDocument3 pagesFamily Health Assessmentkashim123100% (1)
- FNCPDocument2 pagesFNCPNathan MielPas encore d'évaluation
- Community Health Nursing FCPDocument4 pagesCommunity Health Nursing FCPSandeep KumarPas encore d'évaluation
- FNCPDocument5 pagesFNCPHaifi HunPas encore d'évaluation
- Case Study Purok 7Document28 pagesCase Study Purok 7Rhajeeb Aennas SugalaPas encore d'évaluation
- University of Baguio Nursing Students Assess Health of Purok 3Document61 pagesUniversity of Baguio Nursing Students Assess Health of Purok 3Maria MercedesPas encore d'évaluation
- FNCP FinalDocument28 pagesFNCP FinalKristal Jane RuedasPas encore d'évaluation
- Hypertension and Arthritis Health IssuesDocument8 pagesHypertension and Arthritis Health IssuesEunika Castro GarcesPas encore d'évaluation
- ECOMAP Community Health Nursing CHNDocument1 pageECOMAP Community Health Nursing CHNmPas encore d'évaluation
- FNCPDocument3 pagesFNCPHera Pamela Buelis Batoy100% (1)
- Family health issuesDocument9 pagesFamily health issuesShamz SitiarPas encore d'évaluation
- Family Case LoadDocument17 pagesFamily Case LoadFau Fau Dheobo100% (1)
- First Level of AssessmentDocument7 pagesFirst Level of AssessmentJai - Ho100% (1)
- Family Nursing Problems: Breeding Sites, Inadequate Living Space, Health ThreatsDocument1 pageFamily Nursing Problems: Breeding Sites, Inadequate Living Space, Health ThreatsAngeline CasabuenaPas encore d'évaluation
- Cues and Data Family Nursing ProblemsDocument5 pagesCues and Data Family Nursing ProblemsJai - HoPas encore d'évaluation
- Optimize family care with goals, objectives and evaluationDocument21 pagesOptimize family care with goals, objectives and evaluationAnonymous iG0DCOfPas encore d'évaluation
- Family Service and Progress RecordDocument3 pagesFamily Service and Progress RecordKattsurin JyoiPas encore d'évaluation
- Post-abortion pain relief guideDocument7 pagesPost-abortion pain relief guideABDULRAHMAN MISHARI AL-THABITPas encore d'évaluation
- Family Nursing Care Plan (C) SanitationDocument2 pagesFamily Nursing Care Plan (C) SanitationZam Pamate100% (1)
- FNCPDocument10 pagesFNCPMark Jaco AngPas encore d'évaluation
- Typology of Nursing Care ProblemsDocument2 pagesTypology of Nursing Care ProblemsJohnny Yao JrPas encore d'évaluation
- Family Nursing Care Plan InterviewDocument15 pagesFamily Nursing Care Plan InterviewMaurice Ann MarquezPas encore d'évaluation
- Family Caseload Presentation Barangay BalagbagDocument6 pagesFamily Caseload Presentation Barangay BalagbagCharmae NaveaPas encore d'évaluation
- Family Nursing ProcessDocument25 pagesFamily Nursing ProcessJAMES ROD MARINDUQUE100% (1)
- Abella-First Level AssessmentDocument2 pagesAbella-First Level AssessmentWenalyn Grace Abella LlavanPas encore d'évaluation
- FNCP 1Document13 pagesFNCP 1Mikee PeraltaPas encore d'évaluation
- The Chocolate Family: A Case Study of a Filipino Family's Health in Angeles CityDocument75 pagesThe Chocolate Family: A Case Study of a Filipino Family's Health in Angeles CityNat Lynne Distor TrondilloPas encore d'évaluation
- Family Nursing Care Plan: Rationale: To Provide Knowledge About Environmental Sanitation and Its AdvantagesDocument3 pagesFamily Nursing Care Plan: Rationale: To Provide Knowledge About Environmental Sanitation and Its AdvantagesDinarkram Rabreca Ecul100% (1)
- Community Health Nursing for FamiliesDocument24 pagesCommunity Health Nursing for Familiescamel100% (1)
- Initial Data Base For Family Nursing PracticeDocument8 pagesInitial Data Base For Family Nursing PracticeKiara Denise TamayoPas encore d'évaluation
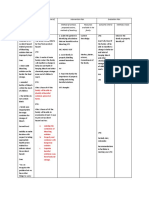
- Family Nursing Care Plan: Khristine Gabrielle U. Robles AND KARLA - 2NU04 GROUPDocument9 pagesFamily Nursing Care Plan: Khristine Gabrielle U. Robles AND KARLA - 2NU04 GROUPEdna Uneta RoblesPas encore d'évaluation
- Family Nursing Care Plan: "Hindi Kasi Uso Sa Kanila Yung Family Planning Eh "Document2 pagesFamily Nursing Care Plan: "Hindi Kasi Uso Sa Kanila Yung Family Planning Eh "Jonver David0% (1)
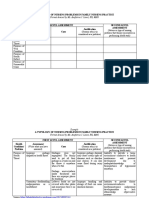
- Typology of Nursing Problems in Family Nursing PracticeDocument2 pagesTypology of Nursing Problems in Family Nursing PracticeHarlene Joyce Rey100% (3)
- Family Nursing Database for April Impit and GrandmotherDocument6 pagesFamily Nursing Database for April Impit and GrandmotherAyaBasilioPas encore d'évaluation
- FNCP AsthmaDocument2 pagesFNCP AsthmaISABELLA MARIE AGUILARPas encore d'évaluation
- FNCP OutputDocument6 pagesFNCP OutputRenz AnggoyPas encore d'évaluation
- TOP 5 HEALTH ISSUESDocument5 pagesTOP 5 HEALTH ISSUESRhiz AntonioPas encore d'évaluation
- Family Nursing Care PlanDocument3 pagesFamily Nursing Care Planmaria yuPas encore d'évaluation
- Family Nursing Care PlanDocument13 pagesFamily Nursing Care PlanClaire AlcantaraPas encore d'évaluation
- CHN FNCPDocument8 pagesCHN FNCPjl frusaPas encore d'évaluation
- Family Nursing Care PlanDocument26 pagesFamily Nursing Care PlanAmira Fatmah QuilapioPas encore d'évaluation
- LackingDocument19 pagesLackingStephen HermosoPas encore d'évaluation
- Final Case Study ManuscriptDocument89 pagesFinal Case Study ManuscriptAlexandra B. FloresPas encore d'évaluation
- CHN Promise Final NaDocument117 pagesCHN Promise Final NaJan Lianne BernalesPas encore d'évaluation
- UntitledDocument2 pagesUntitledRoshwell RegalaPas encore d'évaluation
- Family Health Status and NeedsDocument65 pagesFamily Health Status and NeedsCyrill Alexandria TolentinoPas encore d'évaluation
- Beniga Values Lesson ModuleDocument13 pagesBeniga Values Lesson ModuleRowena BenigaPas encore d'évaluation
- Family Case StudyDocument32 pagesFamily Case StudyRoeder Max PangramuyenPas encore d'évaluation
- Pressing and Finishing (Latest)Document8 pagesPressing and Finishing (Latest)Imran TexPas encore d'évaluation
- Big Band EraDocument248 pagesBig Band Erashiloh32575% (4)
- Komposit UHMWPE Sebagai Alternatif Bantalan Rel Kereta Api: Abel Evan, Alia Kristika, Farid Mulia LatiefDocument11 pagesKomposit UHMWPE Sebagai Alternatif Bantalan Rel Kereta Api: Abel Evan, Alia Kristika, Farid Mulia LatiefAlia KristikaPas encore d'évaluation
- BC Planning EvenDocument5 pagesBC Planning EvenRuth KeziaPas encore d'évaluation
- Gatk Pipeline Presentation: From Fastq Data To High Confident VariantsDocument8 pagesGatk Pipeline Presentation: From Fastq Data To High Confident VariantsSampreeth ReddyPas encore d'évaluation
- EOD Stanags Overview April 2021Document12 pagesEOD Stanags Overview April 2021den mas paratate leo egoPas encore d'évaluation
- Defender 90 110 Workshop Manual 5 WiringDocument112 pagesDefender 90 110 Workshop Manual 5 WiringChris Woodhouse50% (2)
- CELTA Pre-Interview Grammar, Vocabulary and Pronunciation ExercisesDocument4 pagesCELTA Pre-Interview Grammar, Vocabulary and Pronunciation ExercisesMichelJorge100% (2)
- Broom Manufacture Machine: StartDocument62 pagesBroom Manufacture Machine: StartHaziq PazliPas encore d'évaluation
- Scientific Passage English TestDocument57 pagesScientific Passage English TestAb HadiPas encore d'évaluation
- Finding My Voice in ChinatownDocument5 pagesFinding My Voice in ChinatownMagalí MainumbyPas encore d'évaluation
- Literature Review Marketing StrategyDocument4 pagesLiterature Review Marketing Strategyc5td1cmc100% (1)
- SpringDocument4 pagesSpringarun123123Pas encore d'évaluation
- OJT Form 03 Performance EvaluationDocument2 pagesOJT Form 03 Performance EvaluationResshille Ann T. SalleyPas encore d'évaluation
- PMMC ExperimentDocument2 pagesPMMC ExperimentShyam ShankarPas encore d'évaluation
- ENVPEP1412003Document5 pagesENVPEP1412003south adventurePas encore d'évaluation
- Differentiation SS2Document88 pagesDifferentiation SS2merezemenike272Pas encore d'évaluation
- RRR Media Kit April 2018Document12 pagesRRR Media Kit April 2018SilasPas encore d'évaluation
- Rock ClimbingDocument11 pagesRock ClimbingDaria TurdalievaPas encore d'évaluation
- Vivaldi - Genuis of BaroqueDocument279 pagesVivaldi - Genuis of Baroqueilcanto100% (4)
- Albert PikeDocument6 pagesAlbert Pikeapi-302575383Pas encore d'évaluation
- LAU Paleoart Workbook - 2023Document16 pagesLAU Paleoart Workbook - 2023samuelaguilar990Pas encore d'évaluation
- My ResumeDocument4 pagesMy Resumeapi-216740002Pas encore d'évaluation
- Morpho Full Fix 2Document9 pagesMorpho Full Fix 2Dayu AnaPas encore d'évaluation
- BRKSPG-2904-2904 - Cisco Live Session - v2-CL PDFDocument182 pagesBRKSPG-2904-2904 - Cisco Live Session - v2-CL PDFMohamed SamirPas encore d'évaluation
- Project Cost ForecastDocument11 pagesProject Cost ForecastJames MendesPas encore d'évaluation
- Jiangsu Changjiang Electronics Technology Co., Ltd. SOT-89-3L Transistor SpecificationsDocument2 pagesJiangsu Changjiang Electronics Technology Co., Ltd. SOT-89-3L Transistor SpecificationsIsrael AldabaPas encore d'évaluation
- Karan Chawla and Joshua Lee November 21, 2016 MEDS 3020 - Fall 2016 Dr. Rosevear, Dr. Cartwright, Dr. LiebermanDocument2 pagesKaran Chawla and Joshua Lee November 21, 2016 MEDS 3020 - Fall 2016 Dr. Rosevear, Dr. Cartwright, Dr. LiebermanJeremy DelaneyPas encore d'évaluation
- System Software Module 3: Machine-Dependent Assembler FeaturesDocument28 pagesSystem Software Module 3: Machine-Dependent Assembler Featuresvidhya_bineeshPas encore d'évaluation
- Laboratory SafetyDocument4 pagesLaboratory SafetyLey DoydoraPas encore d'évaluation