Vous aimerez peut-être aussi
- Health Issues Caused by Water Pollution To Predict Using Logistic Regression ModelDocument3 pagesHealth Issues Caused by Water Pollution To Predict Using Logistic Regression ModelInternational Journal of Innovative Science and Research TechnologyPas encore d'évaluation
- Vibrio Cholerae - A ReviewDocument7 pagesVibrio Cholerae - A ReviewAlifia Hajar AmandaPas encore d'évaluation
- Trematoda Hati Dan Trematoda UsusDocument46 pagesTrematoda Hati Dan Trematoda UsusIcan DoitPas encore d'évaluation
- CholeraDocument5 pagesCholeralevigojo42Pas encore d'évaluation
- Balantidium Coli PDFDocument15 pagesBalantidium Coli PDFNona MhomedPas encore d'évaluation
- CholeraDocument13 pagesCholerafarida santiPas encore d'évaluation
- Integrated Pest ManagementDocument3 pagesIntegrated Pest Managementvignesh9489Pas encore d'évaluation
- 1 s2.0 S002251931200077X MainDocument8 pages1 s2.0 S002251931200077X MainSudipa ChauhanPas encore d'évaluation
- Mustapha 2013Document8 pagesMustapha 2013Nonika Yassinta SPas encore d'évaluation
- Httpsciteseerx Ist Psu Edudocumentrepid Rep1&Type PDF&Doi Dac388faDocument39 pagesHttpsciteseerx Ist Psu Edudocumentrepid Rep1&Type PDF&Doi Dac388fa98zjwkvysjPas encore d'évaluation
- Cholera - Clinical Features, Diagnosis, Treatment, and Prevention - UpToDateDocument24 pagesCholera - Clinical Features, Diagnosis, Treatment, and Prevention - UpToDate3626issste2020Pas encore d'évaluation
- Vaccine: Sophia Lonappan, Ria Golecha, G. Balakrish NairDocument3 pagesVaccine: Sophia Lonappan, Ria Golecha, G. Balakrish Nairyuniindriani96Pas encore d'évaluation
- Prevalencia H. PyloriDocument4 pagesPrevalencia H. PyloriDonaldo Perez PabloPas encore d'évaluation
- Cholera - Clinical Features, Diagnosis, Treatment, and Prevention - UpToDateDocument35 pagesCholera - Clinical Features, Diagnosis, Treatment, and Prevention - UpToDateMisael TaverasPas encore d'évaluation
- Watkins 2011Document6 pagesWatkins 2011Akiko Syawalidhany TahirPas encore d'évaluation
- Wyn-Jones Et Al 2011 - Surveillance of Adenoviruses and Noroviruses in European Recreational WatersDocument14 pagesWyn-Jones Et Al 2011 - Surveillance of Adenoviruses and Noroviruses in European Recreational WatersYoPas encore d'évaluation
- Pathogens 10 00190Document16 pagesPathogens 10 00190Mariana BarcelóPas encore d'évaluation
- Epidemiology of CholeraDocument10 pagesEpidemiology of CholeraLazy SlothPas encore d'évaluation
- Human Viruses in Water: Perspectives in Medical VirologyD'EverandHuman Viruses in Water: Perspectives in Medical VirologyPas encore d'évaluation
- Guidelines For The Management of Paediatric Cholera Infection: A Systematic Review of The EvidenceDocument16 pagesGuidelines For The Management of Paediatric Cholera Infection: A Systematic Review of The Evidenceمعاذ بامدحجPas encore d'évaluation
- Regional Studies in Marine ScienceDocument9 pagesRegional Studies in Marine ScienceMuns MunnaPas encore d'évaluation
- Infectious Cholera-21 (Muhadharaty)Document7 pagesInfectious Cholera-21 (Muhadharaty)dr.salam.hassaniPas encore d'évaluation
- Disinfection: Handout - Introduction To Drinking Water TreatmentDocument16 pagesDisinfection: Handout - Introduction To Drinking Water TreatmentLeonardo SilvaPas encore d'évaluation
- And Cholera: Vibrio CholeraeDocument30 pagesAnd Cholera: Vibrio CholeraeEddiemtongaPas encore d'évaluation
- Antimicrobial Resistance of Salmonella Species Isolated From Different Environments in Saudi Arabia at Makkah RegionDocument15 pagesAntimicrobial Resistance of Salmonella Species Isolated From Different Environments in Saudi Arabia at Makkah RegionIJAR JOURNALPas encore d'évaluation
- Pone 0235440Document12 pagesPone 0235440Fizza MaryamPas encore d'évaluation
- Vibrio Cholerae Cholera AttackDocument1 pageVibrio Cholerae Cholera AttackAlexandra DolhăscuPas encore d'évaluation
- Associated With Consuming Unsafe Water Through Iced Tea: A Matched Casecontrol StudyDocument18 pagesAssociated With Consuming Unsafe Water Through Iced Tea: A Matched Casecontrol StudySayullys BandaPas encore d'évaluation
- Infection Control For Norovirus: ReviewDocument10 pagesInfection Control For Norovirus: ReviewOfirPas encore d'évaluation
- Effect of Sanitation and Water Treatment On Intestinal Protozoa Infection A Systematic Review and Meta-AnalysisDocument13 pagesEffect of Sanitation and Water Treatment On Intestinal Protozoa Infection A Systematic Review and Meta-AnalysisWiwien HendrawanPas encore d'évaluation
- The Liver Flukes Clonorchis Sinensis OpisthorchisDocument17 pagesThe Liver Flukes Clonorchis Sinensis OpisthorchisDion . APas encore d'évaluation
- The Liver Flukes Clonorchis Sinensis OpisthorchisDocument17 pagesThe Liver Flukes Clonorchis Sinensis OpisthorchisDion . APas encore d'évaluation
- Environmental Microbiology - 2017 - Baker Austin - Vibrio Vulnificus New Insights Into A Deadly Opportunistic PathogenDocument8 pagesEnvironmental Microbiology - 2017 - Baker Austin - Vibrio Vulnificus New Insights Into A Deadly Opportunistic PathogenIggjchthfx JcytxutxutxtjPas encore d'évaluation
- Risk Factors Associated With Typhoid Fever in Children Aged 216 Years in Karachi PakistanDocument8 pagesRisk Factors Associated With Typhoid Fever in Children Aged 216 Years in Karachi Pakistanامتیاز ہاشم بزنجوPas encore d'évaluation
- Vibrio Cholerae From The Environment: Detection, Isolation, and Identification ofDocument51 pagesVibrio Cholerae From The Environment: Detection, Isolation, and Identification ofgiuseppegnrPas encore d'évaluation
- Epidemiology and Control of Communicable Diseases Infections Acquired Through Gastrointestinal TractDocument7 pagesEpidemiology and Control of Communicable Diseases Infections Acquired Through Gastrointestinal TractS APas encore d'évaluation
- 4019.NEJM, GastroentDocument11 pages4019.NEJM, Gastroentbrian.p.lucasPas encore d'évaluation
- (Assignment Name) : "Vibrio Cholerae" Government College of Pharmacy, AurangabadDocument17 pages(Assignment Name) : "Vibrio Cholerae" Government College of Pharmacy, AurangabadGopal KarvaPas encore d'évaluation
- Minireview Escherichia Coli in The Environment: Implications For Water Quality and Human HealthDocument8 pagesMinireview Escherichia Coli in The Environment: Implications For Water Quality and Human HealthTinnysumardiPas encore d'évaluation
- FINALDocument7 pagesFINALDerrickPas encore d'évaluation
- Artikel Rotaviruses FinalDocument30 pagesArtikel Rotaviruses Finalsemangat pagiPas encore d'évaluation
- Intestinal Coccidian: An Overview Epidemiologic Worldwide and ColombiaDocument14 pagesIntestinal Coccidian: An Overview Epidemiologic Worldwide and ColombiaMARIA LUCIA PIESCHACÓN CHUZCANOPas encore d'évaluation
- 1 s2.0 S2090123210000743 Main PDFDocument12 pages1 s2.0 S2090123210000743 Main PDFcamilaPas encore d'évaluation
- WHO SurveillanceVaccinePreventable 02 Cholera R1Document12 pagesWHO SurveillanceVaccinePreventable 02 Cholera R1QaisaramishaPas encore d'évaluation
- Ismi Yunita Sari (K11115524)Document12 pagesIsmi Yunita Sari (K11115524)Ismi Yunita SariPas encore d'évaluation
- Pandemics, Pathogenicity and Changing Molecular Epidemiology of Cholera in The Era of Global WarmingDocument6 pagesPandemics, Pathogenicity and Changing Molecular Epidemiology of Cholera in The Era of Global WarmingAde KurniaPas encore d'évaluation
- JournalDocument13 pagesJournalapi-312404919Pas encore d'évaluation
- Therapy of Acute Gastroenteritis: Role of Antibiotics: ReviewDocument6 pagesTherapy of Acute Gastroenteritis: Role of Antibiotics: ReviewBayuHernawanRahmatMuhariaPas encore d'évaluation
- Free-Living Microorganisms: 5.1 Human Pathogenic Vibrio SpeciesDocument16 pagesFree-Living Microorganisms: 5.1 Human Pathogenic Vibrio SpeciesJin SiclonPas encore d'évaluation
- Severe, Acute Watery Diarrhea in An Adult: Photo QuizDocument4 pagesSevere, Acute Watery Diarrhea in An Adult: Photo Quizfitac_1Pas encore d'évaluation
- Aquaculture: Gastón Higuera, Roberto Bastías, George Tsertsvadze, Jaime Romero, Romilio T. EspejoDocument6 pagesAquaculture: Gastón Higuera, Roberto Bastías, George Tsertsvadze, Jaime Romero, Romilio T. EspejorafaelPas encore d'évaluation
- Communicable DiseasesDocument36 pagesCommunicable DiseasesanaodtohanPas encore d'évaluation
- Vaccine: Neelam Taneja, Arti Mishra, Nitya Batra, Parakriti Gupta, Jaspreet Mahindroo, Balvinder MohanDocument10 pagesVaccine: Neelam Taneja, Arti Mishra, Nitya Batra, Parakriti Gupta, Jaspreet Mahindroo, Balvinder MohanAlexandra DolhăscuPas encore d'évaluation
- Determinants of Full Dose of Oral Cholera Vaccine Uptake in Tiko and Limbe Health DistrictsDocument14 pagesDeterminants of Full Dose of Oral Cholera Vaccine Uptake in Tiko and Limbe Health DistrictsEditor IJTSRDPas encore d'évaluation
- Marine Pollution Bulletin: Sivanandham Vignesh, Krishnan Muthukumar, Rathinam Arthur JamesDocument11 pagesMarine Pollution Bulletin: Sivanandham Vignesh, Krishnan Muthukumar, Rathinam Arthur Jamestatu laurentiuPas encore d'évaluation
- Review: BackgroundDocument11 pagesReview: BackgroundJacqui GCPas encore d'évaluation
- Marine Pollution Bulletin: Sivanandham Vignesh, Krishnan Muthukumar, Rathinam Arthur JamesDocument11 pagesMarine Pollution Bulletin: Sivanandham Vignesh, Krishnan Muthukumar, Rathinam Arthur JamesGeorgiana-LuizaPas encore d'évaluation
- 8 Isolationofa PDFDocument6 pages8 Isolationofa PDFIjaems JournalPas encore d'évaluation
- CholeraDocument11 pagesCholeraJanisPas encore d'évaluation
- Cyclospora and Cyclosporiasis: Epidemiology, Diagnosis, Detection, and ControlD'EverandCyclospora and Cyclosporiasis: Epidemiology, Diagnosis, Detection, and ControlPas encore d'évaluation
- Research Project Plan RP10-03 Urinary Incontinence Among Dependent Women and Men Over 80 Years in Relation To Staff Attitudes and KnowledgeDocument5 pagesResearch Project Plan RP10-03 Urinary Incontinence Among Dependent Women and Men Over 80 Years in Relation To Staff Attitudes and KnowledgeNurul HafizaPas encore d'évaluation
- Aop047 12-Sci1219 PDFDocument6 pagesAop047 12-Sci1219 PDFNurul HafizaPas encore d'évaluation
- Daftar PustakaDocument5 pagesDaftar PustakaNurul HafizaPas encore d'évaluation
- Patients' Experience of Living With Glaucoma: A Phenomenological StudyDocument11 pagesPatients' Experience of Living With Glaucoma: A Phenomenological StudyNurul HafizaPas encore d'évaluation
- Urinary Incontinence in The Older Adult: by Kristen Cook, Pharm.D., BCPS and Linda M. Sobeski, Pharm.D., BCPSDocument18 pagesUrinary Incontinence in The Older Adult: by Kristen Cook, Pharm.D., BCPS and Linda M. Sobeski, Pharm.D., BCPSNurul HafizaPas encore d'évaluation
- 18 Bicer Original 10 1Document8 pages18 Bicer Original 10 1Nurul HafizaPas encore d'évaluation
- 2 1 1 SMDocument6 pages2 1 1 SMNurul HafizaPas encore d'évaluation
- J.S.S College of Nursing 1 Main Saraswathipuram, MysoreDocument18 pagesJ.S.S College of Nursing 1 Main Saraswathipuram, MysoreNurul HafizaPas encore d'évaluation
- 1 s2.0 S1347861316300251 MainDocument107 pages1 s2.0 S1347861316300251 MainNurul HafizaPas encore d'évaluation
- Out 8Document8 pagesOut 8Nurul HafizaPas encore d'évaluation
- Day 11 PDFDocument16 pagesDay 11 PDFჯონ ფრაატეეკPas encore d'évaluation
- HS ĐỀ CƯƠNG KIỂM TRA GIỮA KỲ I KHOI 10 NH 23 24Document6 pagesHS ĐỀ CƯƠNG KIỂM TRA GIỮA KỲ I KHOI 10 NH 23 24Ngô Hiểu NhiênPas encore d'évaluation
- Internship Report On Service IndustryDocument50 pagesInternship Report On Service Industrybbaahmad89Pas encore d'évaluation
- Reference GuideDocument3 pagesReference GuideStudentforiPas encore d'évaluation
- To Determine The Minimum Transportation Cost by Comparing The Initial Basic Feasible Solution of A Transportation Problem by Various MethodsDocument3 pagesTo Determine The Minimum Transportation Cost by Comparing The Initial Basic Feasible Solution of A Transportation Problem by Various MethodsInternational Journal of Innovative Science and Research TechnologyPas encore d'évaluation
- IRJES 2017 Vol. 1 Special Issue 2 English Full Paper 038Document6 pagesIRJES 2017 Vol. 1 Special Issue 2 English Full Paper 038liew wei keongPas encore d'évaluation
- Charity Connecting System: M.Archana, K.MouthamiDocument5 pagesCharity Connecting System: M.Archana, K.MouthamiShainara Dela TorrePas encore d'évaluation
- Vertical Axis Wind Turbine ProjDocument2 pagesVertical Axis Wind Turbine Projmacsan sanchezPas encore d'évaluation
- Jenkins Course Slides PDFDocument96 pagesJenkins Course Slides PDFkamal.tejnani5613100% (2)
- The Structure of Deception: Validation of The Lying Profile QuestionnaireDocument16 pagesThe Structure of Deception: Validation of The Lying Profile QuestionnaireNancy DrewPas encore d'évaluation
- Project Guidelines: (A Manual For Preparation of Project Report)Document4 pagesProject Guidelines: (A Manual For Preparation of Project Report)Shivam TiwariPas encore d'évaluation
- Unit 9 Caring and Sharing Year 2 KSSR Lesson PlanDocument6 pagesUnit 9 Caring and Sharing Year 2 KSSR Lesson PlanopheliavioletPas encore d'évaluation
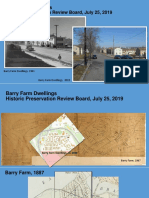
- Barry Farm Powerpoint SlidesDocument33 pagesBarry Farm Powerpoint SlidessarahPas encore d'évaluation
- For Purposeful and Meaningful Technology Integration in The ClassroomDocument19 pagesFor Purposeful and Meaningful Technology Integration in The ClassroomVincent Chris Ellis TumalePas encore d'évaluation
- Potential Application of Orange Peel (OP) As An Eco-Friendly Adsorbent For Textile Dyeing EffluentsDocument13 pagesPotential Application of Orange Peel (OP) As An Eco-Friendly Adsorbent For Textile Dyeing EffluentsAnoif Naputo AidnamPas encore d'évaluation
- SLC 10 ScienceDocument16 pagesSLC 10 SciencePffflyers KurnawanPas encore d'évaluation
- EC861Document10 pagesEC861damaiPas encore d'évaluation
- Fidelizer Pro User GuideDocument12 pagesFidelizer Pro User GuidempptritanPas encore d'évaluation
- Agents SocializationDocument4 pagesAgents Socializationinstinct920% (1)
- Role of Wickability On The Critical Heat Flux of Structured Superhydrophilic SurfacesDocument10 pagesRole of Wickability On The Critical Heat Flux of Structured Superhydrophilic Surfacesavi0341Pas encore d'évaluation
- DSpace Configuration PDFDocument1 pageDSpace Configuration PDFArshad SanwalPas encore d'évaluation
- Comparision BRC IFS QMS 22K From BV PDFDocument44 pagesComparision BRC IFS QMS 22K From BV PDFAhmedElSayedPas encore d'évaluation
- Naeyc StandardsDocument11 pagesNaeyc Standardsapi-266968546Pas encore d'évaluation
- Bab 4 Ba501 Pecahan SeparaDocument24 pagesBab 4 Ba501 Pecahan SeparaPrince ShanPas encore d'évaluation
- SYLLABUS For DRAW 122Document7 pagesSYLLABUS For DRAW 122Alther Dabon0% (1)
- USACODocument94 pagesUSACOLyokoPotterPas encore d'évaluation
- Policy Analysis ReportDocument16 pagesPolicy Analysis ReportGhelvin Auriele AguirrePas encore d'évaluation
- Unification of Euler and Werner Deconvolution in Three Dimensions Via The Generalized Hilbert TransformDocument6 pagesUnification of Euler and Werner Deconvolution in Three Dimensions Via The Generalized Hilbert TransformMithunPas encore d'évaluation
- Fichas Slate HoneywellDocument1 pageFichas Slate HoneywellING CARLOS RAMOSPas encore d'évaluation