Vous aimerez peut-être aussi
- Diagnosis and Management of Cholangiocarcinoma: A Multidisciplinary ApproachD'EverandDiagnosis and Management of Cholangiocarcinoma: A Multidisciplinary ApproachJames H. TabibianPas encore d'évaluation
- Histopathology of Hepatocellular CarcinomaDocument11 pagesHistopathology of Hepatocellular CarcinomaCindy Sabina FaleandraPas encore d'évaluation
- hepatoCA 2Document9 pageshepatoCA 2Al VlaovicPas encore d'évaluation
- Seminar: Arndt Vogel, Tim Meyer, Gonzalo Sapisochin, Riad Salem, Anna SaborowskiDocument18 pagesSeminar: Arndt Vogel, Tim Meyer, Gonzalo Sapisochin, Riad Salem, Anna SaborowskiKarolinakuprescenkaitePas encore d'évaluation
- Hepatocellular Carcinoma: Clinical Frontiers and PerspectivesDocument13 pagesHepatocellular Carcinoma: Clinical Frontiers and PerspectivesMisnariahIdrusPas encore d'évaluation
- Hepatocellular CarcinomaDocument18 pagesHepatocellular CarcinomaIngrid González EfronPas encore d'évaluation
- Colon CancerDocument10 pagesColon CancerHerlina TanPas encore d'évaluation
- Diagnosis of Hepatocellular CarcinomaDocument13 pagesDiagnosis of Hepatocellular CarcinomaOana AndreeaPas encore d'évaluation
- Biochemical Markers of Colorectal Cancer Present and FutureDocument10 pagesBiochemical Markers of Colorectal Cancer Present and FutureMarcellia AngelinaPas encore d'évaluation
- Development and Novel Therapeutics in Hepatocellular Carcinoma A ReviewDocument11 pagesDevelopment and Novel Therapeutics in Hepatocellular Carcinoma A ReviewgrigmihPas encore d'évaluation
- Malignant Liver Tumours: Table 1Document8 pagesMalignant Liver Tumours: Table 1abbasPas encore d'évaluation
- Zhu 2011Document11 pagesZhu 2011nurulailiPas encore d'évaluation
- Forner Lancet 2012 HccreviewDocument11 pagesForner Lancet 2012 Hccreviewapi-283759086Pas encore d'évaluation
- Hepato CA 8Document15 pagesHepato CA 8Al VlaovicPas encore d'évaluation
- Haake Et Al 2017 CancerDocument10 pagesHaake Et Al 2017 Cancerdiego peinadoPas encore d'évaluation
- Liver Cancer Research PaperDocument8 pagesLiver Cancer Research Papernywxluvkg100% (1)
- Applications and StrategiesDocument16 pagesApplications and StrategiesMariaAlejandraChanciPas encore d'évaluation
- Hayes 2015Document10 pagesHayes 2015Victor CoutinhoPas encore d'évaluation
- Jurnal Ricky 2Document24 pagesJurnal Ricky 2Dyki AnwarPas encore d'évaluation
- Pancreatic Cancer: A Review of Risk Factors, Diagnosis, and TreatmentDocument13 pagesPancreatic Cancer: A Review of Risk Factors, Diagnosis, and TreatmentNoy FaridaPas encore d'évaluation
- Pediatric Hepatocelullar CarcinomaDocument21 pagesPediatric Hepatocelullar Carcinomamoh.ikhsanzPas encore d'évaluation
- Epidemiology and Screening For Renal CancerDocument14 pagesEpidemiology and Screening For Renal CancermicozaaaPas encore d'évaluation
- Testicular Cancer NCCN2015Document28 pagesTesticular Cancer NCCN2015palomazul007Pas encore d'évaluation
- Metastasis Site Liver CancerDocument7 pagesMetastasis Site Liver CancerChristofel JomanPas encore d'évaluation
- Prostate Cancer: Key PointsDocument4 pagesProstate Cancer: Key PointsGabriel ŞarguPas encore d'évaluation
- Kidney Cancer: Radiology and Oncology June 2007Document9 pagesKidney Cancer: Radiology and Oncology June 2007aaaaPas encore d'évaluation
- Circulating Cell-Free DNA or Circulating Tumor DNA in The Management of Ovarian and Endometrial CancerDocument14 pagesCirculating Cell-Free DNA or Circulating Tumor DNA in The Management of Ovarian and Endometrial CancerSergio J Calleja FreixesPas encore d'évaluation
- HNCReview 2014Document13 pagesHNCReview 2014Muzammil Ahmad QureshiPas encore d'évaluation
- 1 PBDocument6 pages1 PBGhiban ConstantinPas encore d'évaluation
- 624 PDFDocument9 pages624 PDFTri AryantiPas encore d'évaluation
- Testis CancerDocument9 pagesTestis CancerMuhammad Tawfiq ZamriPas encore d'évaluation
- Jurnal Kanker TestisDocument9 pagesJurnal Kanker TestisDiatni FibriPas encore d'évaluation
- Primer: Hepatocellular CarcinomaDocument28 pagesPrimer: Hepatocellular CarcinomaAinun Aii NoorPas encore d'évaluation
- Advancing On Pancreatic CancerDocument1 pageAdvancing On Pancreatic CancermohamedPas encore d'évaluation
- Pancreatic CancerDocument14 pagesPancreatic Cancerpaulo saPas encore d'évaluation
- Rare Kidney Tumors Comprehensive Multidisciplinary Management and Emerging TherapiesDocument131 pagesRare Kidney Tumors Comprehensive Multidisciplinary Management and Emerging TherapiesAd AdrianaPas encore d'évaluation
- HHS Public Access: Author ManuscriptDocument26 pagesHHS Public Access: Author ManuscriptCherryPas encore d'évaluation
- Neoplasia and Cancer: Week 1Document8 pagesNeoplasia and Cancer: Week 1rise wiiinPas encore d'évaluation
- 2020 Paper SplenicDocument5 pages2020 Paper SplenicLauburu CrossPas encore d'évaluation
- hepatoCA 7Document15 pageshepatoCA 7Al VlaovicPas encore d'évaluation
- Zebra FishDocument552 pagesZebra FishmcvalledorPas encore d'évaluation
- Managementul Cancerului Colorec TalDocument6 pagesManagementul Cancerului Colorec TalDiana BlanaruPas encore d'évaluation
- Oncotarget MC Mullen Selleck Senthil 2017Document11 pagesOncotarget MC Mullen Selleck Senthil 2017fitriaokPas encore d'évaluation
- Beta-Blocker Drug Use and Survival Among Patients With Pancreatic AdenocarcinomaDocument9 pagesBeta-Blocker Drug Use and Survival Among Patients With Pancreatic AdenocarcinomaHao LiuPas encore d'évaluation
- Cancer Stem Cells With Increased Metastatic Potential As - 2017 - Seminars in CaDocument7 pagesCancer Stem Cells With Increased Metastatic Potential As - 2017 - Seminars in CaFlorin AchimPas encore d'évaluation
- Adenomatous Polyps of The Colon 2006Document7 pagesAdenomatous Polyps of The Colon 2006Anelise SchaedlerPas encore d'évaluation
- Liver Tumors - Epidemiology, Diagnosis, Prevention and Treatment (Helen Reeves)Document184 pagesLiver Tumors - Epidemiology, Diagnosis, Prevention and Treatment (Helen Reeves)JohnQPas encore d'évaluation
- Circulating Endothelial Cells and Other Angiogenesis Factors in Pancreatic Carcinoma Patients Receiving Gemcitabine ChemotherapyDocument10 pagesCirculating Endothelial Cells and Other Angiogenesis Factors in Pancreatic Carcinoma Patients Receiving Gemcitabine ChemotherapyftwPas encore d'évaluation
- 2009 0527 rs.1 PDFDocument5 pages2009 0527 rs.1 PDFpaolaPas encore d'évaluation
- Kuipersetal CRC NRDP2015Document26 pagesKuipersetal CRC NRDP2015Robert ChristevenPas encore d'évaluation
- 8-PIK3 Head and Neck ReviewDocument14 pages8-PIK3 Head and Neck ReviewNgan Wei PinPas encore d'évaluation
- MEHU130 U2 T74 Colorectal CancerDocument14 pagesMEHU130 U2 T74 Colorectal CancerStefani AtllePas encore d'évaluation
- Causes of Cancer What To Know About CancerDocument4 pagesCauses of Cancer What To Know About CancerfinlandthelandoficePas encore d'évaluation
- JurnalDocument8 pagesJurnalAriefPratamaPas encore d'évaluation
- Colon CancerDocument7 pagesColon CancerKen Ancheta LagayadaPas encore d'évaluation
- Cancer and Liver Cirrhosis: Implications On Prognosis and ManagementDocument16 pagesCancer and Liver Cirrhosis: Implications On Prognosis and ManagementAlifia Ramadhanty PrameswariPas encore d'évaluation
- Review Article: Biomarkers For Hepatocellular CarcinomaDocument8 pagesReview Article: Biomarkers For Hepatocellular CarcinomaAya AlkaffPas encore d'évaluation
- Fibrolamellar Variant of Hepatocellular Carcinoma in A Young FemaleDocument3 pagesFibrolamellar Variant of Hepatocellular Carcinoma in A Young FemaleIKIKIKIKIKI999999Pas encore d'évaluation
- ESMO Clinical PracticeDocument13 pagesESMO Clinical PracticePati MuresanPas encore d'évaluation
- Malignant Liver Tumours OxfordDocument7 pagesMalignant Liver Tumours OxfordJose Tomás MoorePas encore d'évaluation
- PRE-BOARD EXAMINATION, January 2015 Class XII Biology (044) : G.G.N. Public School, Rose Garden, LudhianaDocument5 pagesPRE-BOARD EXAMINATION, January 2015 Class XII Biology (044) : G.G.N. Public School, Rose Garden, LudhianaSamita BhallaPas encore d'évaluation
- Amyotrophic Lateral SclerosisDocument11 pagesAmyotrophic Lateral SclerosisAnomalie12345Pas encore d'évaluation
- Biology TipsDocument160 pagesBiology TipsAnonymous CaiIz7Nw34Pas encore d'évaluation
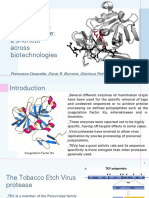
- Tobacco Etch Virus Protease: A Shortcut Across BiotechnologiesDocument16 pagesTobacco Etch Virus Protease: A Shortcut Across BiotechnologiesNhật ThiệnPas encore d'évaluation
- Introduction To Metabolism: Dr. Md. Rageeb Md. Usman Associate Professor Department of PharmacognosyDocument13 pagesIntroduction To Metabolism: Dr. Md. Rageeb Md. Usman Associate Professor Department of PharmacognosyAnonymous TCbZigVqPas encore d'évaluation
- THE Process of DigestionDocument39 pagesTHE Process of Digestionskaii100% (1)
- Molecules: The New Challenge of Green Cosmetics: Natural Food Ingredients For Cosmetic FormulationsDocument28 pagesMolecules: The New Challenge of Green Cosmetics: Natural Food Ingredients For Cosmetic FormulationsalbertoPas encore d'évaluation
- Biology Chapter 1 Notes (Grade 11)Document4 pagesBiology Chapter 1 Notes (Grade 11)Tammy Lam100% (11)
- Genetic Basis of Inheritance-FinalPDFDocument16 pagesGenetic Basis of Inheritance-FinalPDFknlsinhaPas encore d'évaluation
- VC Online Refresher 2017Document32 pagesVC Online Refresher 2017Angela Garcia50% (4)
- Cell SpecializationDocument21 pagesCell SpecializationMatt NupenPas encore d'évaluation
- Glycogen Storage DiseasesDocument7 pagesGlycogen Storage DiseasesNikhilBhattPas encore d'évaluation
- Gay LesbianDocument17 pagesGay LesbianFarhat JabeenPas encore d'évaluation
- PCR LectureDocument35 pagesPCR LectureArfan Tri KusumaPas encore d'évaluation
- Genbio2 Week 2 2Document44 pagesGenbio2 Week 2 2kimberlyfritzzunigaPas encore d'évaluation
- Helicobacter PyloriDocument42 pagesHelicobacter Pyloritummalapalli venkateswara raoPas encore d'évaluation
- Bioinformatics DefinitionDocument11 pagesBioinformatics DefinitionsubinPas encore d'évaluation
- Pune Stem Cell Meet - 2011 - Dr. Rao PapineniDocument10 pagesPune Stem Cell Meet - 2011 - Dr. Rao PapineniPapineni LabsPas encore d'évaluation
- TestBank ch01Document25 pagesTestBank ch01Edison BajramajPas encore d'évaluation
- Maxima H Minus First Strand cDNA Synthesis Kit: Thermo ScientificDocument2 pagesMaxima H Minus First Strand cDNA Synthesis Kit: Thermo ScientificEmily AguirrePas encore d'évaluation
- CH - 2 - Reproduction in Flowering Plants - L-1Document23 pagesCH - 2 - Reproduction in Flowering Plants - L-1yashPas encore d'évaluation
- Kuliah Umum TransfusiDocument54 pagesKuliah Umum TransfusiAnton TriyadiPas encore d'évaluation
- Review SheetDocument2 pagesReview Sheetapi-289866381Pas encore d'évaluation
- Determinants of HealthDocument29 pagesDeterminants of HealthMayom MabuongPas encore d'évaluation
- Environmental Science SyllabusDocument5 pagesEnvironmental Science Syllabusapi-262589183Pas encore d'évaluation
- Course Catalogue 21 22 UpdatedDocument286 pagesCourse Catalogue 21 22 UpdatedKumarPas encore d'évaluation
- BiodiversityDocument94 pagesBiodiversitySaif Mohammad100% (1)
- Question Bank For Telangana State Board BiologyDocument105 pagesQuestion Bank For Telangana State Board BiologyChetan JainPas encore d'évaluation
- Biological KingdomsDocument2 pagesBiological KingdomsValeria GrijalvaPas encore d'évaluation
- Research Project Proposals: Date PublishedDocument14 pagesResearch Project Proposals: Date PublishedJaylord AgpuldoPas encore d'évaluation