Vous aimerez peut-être aussi
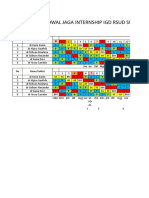
- Jadwal Jaga Internship IGD RSUD SumedangDocument3 pagesJadwal Jaga Internship IGD RSUD SumedangKevin KarimPas encore d'évaluation
- Approach To The Patient With Fever EditedDocument72 pagesApproach To The Patient With Fever EditedKevin Karim100% (1)
- By Thamrin Syamsudin, DR., SP.S (K)Document37 pagesBy Thamrin Syamsudin, DR., SP.S (K)Kevin KarimPas encore d'évaluation
- SitasiDocument2 pagesSitasiKevin KarimPas encore d'évaluation
- Women, Renal Disease and PregnancyDocument16 pagesWomen, Renal Disease and PregnancyKevin KarimPas encore d'évaluation
- PAIN P3D Baru Dr. YWDocument59 pagesPAIN P3D Baru Dr. YWKevin KarimPas encore d'évaluation
- P3D 2011 Dr. HASDocument42 pagesP3D 2011 Dr. HASKevin KarimPas encore d'évaluation
- SitasiDocument2 pagesSitasiKevin KarimPas encore d'évaluation
- CNS Infections Diagnosis and TreatmentDocument57 pagesCNS Infections Diagnosis and TreatmentKevin KarimPas encore d'évaluation
- Stroke & VertigoDocument84 pagesStroke & VertigoAdisti Erlina SutomoPas encore d'évaluation
- Maternal Deaths in Women With Lupus Nephritis - A Review of Published EvidenceDocument8 pagesMaternal Deaths in Women With Lupus Nephritis - A Review of Published EvidenceKevin KarimPas encore d'évaluation
- WHO-SEARO Snakebite Guidelines 2010Document162 pagesWHO-SEARO Snakebite Guidelines 2010Galantry Ahmad AzhariPas encore d'évaluation
- Sir OsisDocument31 pagesSir OsisKevin KarimPas encore d'évaluation
- Jadwal Puskesmas Baru FIXXXXDocument14 pagesJadwal Puskesmas Baru FIXXXXKevin KarimPas encore d'évaluation
- Pregnancy With Lupus Nephritis - A Case ReportDocument3 pagesPregnancy With Lupus Nephritis - A Case ReportKevin KarimPas encore d'évaluation
- PR ThoraksDocument19 pagesPR ThoraksKevin KarimPas encore d'évaluation
- Effect of Gender On Clinical Presentation in Systemic Lupus ErythematosusDocument8 pagesEffect of Gender On Clinical Presentation in Systemic Lupus ErythematosusKevin KarimPas encore d'évaluation
- Sir OsisDocument31 pagesSir OsisKevin KarimPas encore d'évaluation
- Buerger's Disease: A Presentation by Jennifer Kent-BakerDocument14 pagesBuerger's Disease: A Presentation by Jennifer Kent-BakerKevin KarimPas encore d'évaluation
- CSS - Nabil Lisbeth VitriDocument70 pagesCSS - Nabil Lisbeth VitriKevin KarimPas encore d'évaluation
- Gout ArthritisDocument39 pagesGout ArthritisKevin KarimPas encore d'évaluation
- Gout ArthritisDocument39 pagesGout ArthritisKevin KarimPas encore d'évaluation
- Kuliah Retina p3d RevDocument61 pagesKuliah Retina p3d RevKevin KarimPas encore d'évaluation
- PR ThoraksDocument19 pagesPR ThoraksKevin KarimPas encore d'évaluation
- Visual Pathway & Binocular Vision: DR Feti Karfiati, DR, SPM (K), MkesDocument36 pagesVisual Pathway & Binocular Vision: DR Feti Karfiati, DR, SPM (K), MkesKevin KarimPas encore d'évaluation
- Principles of Fractures: (Compound) Fracture, Liable To Contamination and InfectionDocument1 pagePrinciples of Fractures: (Compound) Fracture, Liable To Contamination and InfectionEnggar Adi NugrohoPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Resarch Paper On Franchising Business MacobDocument8 pagesResarch Paper On Franchising Business MacobAngelika Capa ReyesPas encore d'évaluation
- Business Law Module No. 2Document10 pagesBusiness Law Module No. 2Yolly DiazPas encore d'évaluation
- Edition 100Document30 pagesEdition 100Tockington Manor SchoolPas encore d'évaluation
- Manila Pilots Association Immune from Attachment for Member's DebtDocument2 pagesManila Pilots Association Immune from Attachment for Member's DebtAngelic ArcherPas encore d'évaluation
- Compro Russindo Group Tahun 2018 UpdateDocument44 pagesCompro Russindo Group Tahun 2018 UpdateElyza Farah FadhillahPas encore d'évaluation
- Food Product Development - SurveyDocument4 pagesFood Product Development - SurveyJoan Soliven33% (3)
- Introduction to History Part 1: Key ConceptsDocument32 pagesIntroduction to History Part 1: Key ConceptsMaryam14xPas encore d'évaluation
- Corporate Law Scope and RegulationDocument21 pagesCorporate Law Scope and RegulationBasit KhanPas encore d'évaluation
- Tadesse JaletaDocument160 pagesTadesse JaletaAhmed GemedaPas encore d'évaluation
- Brain Chip ReportDocument30 pagesBrain Chip Reportsrikanthkalemla100% (3)
- The Neteru Gods Goddesses of The Grand EnneadDocument16 pagesThe Neteru Gods Goddesses of The Grand EnneadKirk Teasley100% (1)
- Skin Yale University Protein: Where Does Collagen Come From?Document2 pagesSkin Yale University Protein: Where Does Collagen Come From?Ellaine Pearl AlmillaPas encore d'évaluation
- Barra de Pinos 90G 2x5 P. 2,54mm - WE 612 010 217 21Document2 pagesBarra de Pinos 90G 2x5 P. 2,54mm - WE 612 010 217 21Conrado Almeida De OliveiraPas encore d'évaluation
- Autos MalaysiaDocument45 pagesAutos MalaysiaNicholas AngPas encore d'évaluation
- Vegan Banana Bread Pancakes With Chocolate Chunks Recipe + VideoDocument33 pagesVegan Banana Bread Pancakes With Chocolate Chunks Recipe + VideoGiuliana FloresPas encore d'évaluation
- FM Stereo FM-AM Tuner: ST-SE500 ST-SE700Document64 pagesFM Stereo FM-AM Tuner: ST-SE500 ST-SE700al80al80100% (4)
- Battery Genset Usage 06-08pelj0910Document4 pagesBattery Genset Usage 06-08pelj0910b400013Pas encore d'évaluation
- RA 4196 University Charter of PLMDocument4 pagesRA 4196 University Charter of PLMJoan PabloPas encore d'évaluation
- Labov-DIFUSÃO - Resolving The Neogrammarian ControversyDocument43 pagesLabov-DIFUSÃO - Resolving The Neogrammarian ControversyGermana RodriguesPas encore d'évaluation
- La TraviataDocument12 pagesLa TraviataEljona YzellariPas encore d'évaluation
- International Standard Knowledge Olympiad - Exam Syllabus Eligibility: Class 1-10 Class - 1Document10 pagesInternational Standard Knowledge Olympiad - Exam Syllabus Eligibility: Class 1-10 Class - 1V A Prem KumarPas encore d'évaluation
- Opportunity, Not Threat: Crypto AssetsDocument9 pagesOpportunity, Not Threat: Crypto AssetsTrophy NcPas encore d'évaluation
- Topic 1 in 21st CneturyDocument8 pagesTopic 1 in 21st CneturyLuwisa RamosPas encore d'évaluation
- ACS Tech Manual Rev9 Vol1-TACTICS PDFDocument186 pagesACS Tech Manual Rev9 Vol1-TACTICS PDFMihaela PecaPas encore d'évaluation
- ms3 Seq 01 Expressing Interests With Adverbs of FrequencyDocument3 pagesms3 Seq 01 Expressing Interests With Adverbs of Frequencyg27rimaPas encore d'évaluation
- University of Wisconsin Proposal TemplateDocument5 pagesUniversity of Wisconsin Proposal TemplateLuke TilleyPas encore d'évaluation
- Java Interview Questions: Interfaces, Abstract Classes, Overloading, OverridingDocument2 pagesJava Interview Questions: Interfaces, Abstract Classes, Overloading, OverridingGopal JoshiPas encore d'évaluation
- The Awesome Life Force 1984Document8 pagesThe Awesome Life Force 1984Roman PetersonPas encore d'évaluation
- Arx Occasional Papers - Hospitaller Gunpowder MagazinesDocument76 pagesArx Occasional Papers - Hospitaller Gunpowder MagazinesJohn Spiteri GingellPas encore d'évaluation
- Tes 1 KunciDocument5 pagesTes 1 Kuncieko riyadiPas encore d'évaluation