Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- George Floyd Autopsy (FULL REPORT)Document20 pagesGeorge Floyd Autopsy (FULL REPORT)Law&Crime91% (56)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Criminal Complaint For Nicolae MiuDocument9 pagesCriminal Complaint For Nicolae MiuPatch Minnesota100% (3)
- 911-Transcripts 22-159398 13.82 RedactedDocument13 pages911-Transcripts 22-159398 13.82 RedactedPatch Minnesota100% (2)
- Minnesota Work Zone Speed Management Study 2022Document72 pagesMinnesota Work Zone Speed Management Study 2022Patch MinnesotaPas encore d'évaluation
- Minneapolis Mayor Isareal-Hamas ProclamationDocument2 pagesMinneapolis Mayor Isareal-Hamas ProclamationPatch MinnesotaPas encore d'évaluation
- Addison Citation SummaryDocument1 pageAddison Citation SummaryPatch MinnesotaPas encore d'évaluation
- Gooden, Shannon CortezDocument1 pageGooden, Shannon CortezPatch MinnesotaPas encore d'évaluation
- Search WarrantDocument7 pagesSearch WarrantPatch MinnesotaPas encore d'évaluation
- Shannon Gooden Search WarrantDocument9 pagesShannon Gooden Search WarrantPatch MinnesotaPas encore d'évaluation
- Letter From FLI - RedactedDocument11 pagesLetter From FLI - RedactedPatch MinnesotaPas encore d'évaluation
- Everson Griffen Citation Data SummaryDocument2 pagesEverson Griffen Citation Data SummaryPatch MinnesotaPas encore d'évaluation
- Jackie Rahm Little, 36, Cash BailDocument1 pageJackie Rahm Little, 36, Cash BailPatch MinnesotaPas encore d'évaluation
- Ralph Leslie ApmannDocument7 pagesRalph Leslie ApmannPatch MinnesotaPas encore d'évaluation
- Order - Dismiss - Not Stipulated, Entire CaseDocument4 pagesOrder - Dismiss - Not Stipulated, Entire CasePatch MinnesotaPas encore d'évaluation
- Gov. Tim Walz Kids and Families Budget ProposalDocument10 pagesGov. Tim Walz Kids and Families Budget ProposalPatch MinnesotaPas encore d'évaluation
- Petition Matthew HillDocument7 pagesPetition Matthew HillPatch MinnesotaPas encore d'évaluation
- HF0100.0 - MinnesotaDocument302 pagesHF0100.0 - MinnesotaPatch MinnesotaPas encore d'évaluation
- Minnesota - 2021 No Knock Annual ReportDocument20 pagesMinnesota - 2021 No Knock Annual ReportPatch Minnesota100% (1)
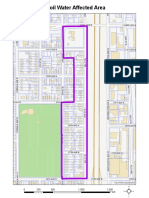
- Boil Water Affected Area - MinneapolisDocument1 pageBoil Water Affected Area - MinneapolisPatch MinnesotaPas encore d'évaluation
- 2023 One Minnesota Budget Fact SheetDocument4 pages2023 One Minnesota Budget Fact SheetWCCO - CBS MinnesotaPas encore d'évaluation
- Holmes, Nosakhere - Petition - 2.14.23Document6 pagesHolmes, Nosakhere - Petition - 2.14.23Patch MinnesotaPas encore d'évaluation
- MCRO - 27-CV-21-9182 - Amended Summons and Complaint - 2021-07-27 - 20221205114459Document22 pagesMCRO - 27-CV-21-9182 - Amended Summons and Complaint - 2021-07-27 - 20221205114459Patch MinnesotaPas encore d'évaluation
- Verdict in Alfredo Rosario Solis TrialDocument12 pagesVerdict in Alfredo Rosario Solis TrialPatch MinnesotaPas encore d'évaluation
- Shipt Summons ComplaintDocument58 pagesShipt Summons ComplaintPatch MinnesotaPas encore d'évaluation
- Lawsuit Filed by Chyna Whitaker Against Ben Crump, Katie WrightDocument19 pagesLawsuit Filed by Chyna Whitaker Against Ben Crump, Katie WrightPatch MinnesotaPas encore d'évaluation
- Federal Case of Bratjan Frank Jr.Document12 pagesFederal Case of Bratjan Frank Jr.Patch MinnesotaPas encore d'évaluation
- Mohamed Ali Selim - Petition To Enter Guilty PleaDocument5 pagesMohamed Ali Selim - Petition To Enter Guilty PleaPatch MinnesotaPas encore d'évaluation
- MCRO - 62 CV 20 5492 - Order Other - 2021 06 24 - 20220923175955Document8 pagesMCRO - 62 CV 20 5492 - Order Other - 2021 06 24 - 20220923175955Scott JohnsonPas encore d'évaluation
- Minnesota Abortion Ruling 2022Document140 pagesMinnesota Abortion Ruling 2022Patch MinnesotaPas encore d'évaluation
- Minnesota State Patrol - DWI ArrestsDocument7 pagesMinnesota State Patrol - DWI ArrestsPatch MinnesotaPas encore d'évaluation