Vous aimerez peut-être aussi
- APBHPDocument35 pagesAPBHPDonna Lei G. RosarioPas encore d'évaluation
- Journal Analysis-BALLON, Karlo CDocument4 pagesJournal Analysis-BALLON, Karlo CMelinda Cariño BallonPas encore d'évaluation
- Family Nursing Care PlanDocument14 pagesFamily Nursing Care PlanTenth Ann ModanzaPas encore d'évaluation
- Module 3 CHN 1Document4 pagesModule 3 CHN 1Danz Kie100% (1)
- Problem Identification and PrioritizationDocument8 pagesProblem Identification and PrioritizationStudent FilesPas encore d'évaluation
- CHNDocument8 pagesCHNAziil LiizaPas encore d'évaluation
- E. Nursing DiagnosisDocument2 pagesE. Nursing DiagnosisAle SandraPas encore d'évaluation
- Topic 1: Introduction To Geria Nursing: Activity 1.1: Grandparents' LoveDocument11 pagesTopic 1: Introduction To Geria Nursing: Activity 1.1: Grandparents' LoveMarissa AsimPas encore d'évaluation
- Biopsy: Assessment Diagnosis Planning Intervention Rationale EvaluationDocument5 pagesBiopsy: Assessment Diagnosis Planning Intervention Rationale EvaluationDan HizonPas encore d'évaluation
- Community Health Nursing Board ExamDocument9 pagesCommunity Health Nursing Board ExamFermin K. CuasitoPas encore d'évaluation
- National Leprosy Control Program For CHNDocument18 pagesNational Leprosy Control Program For CHNNaomi Cyden YapPas encore d'évaluation
- Funda ReviewerDocument8 pagesFunda ReviewerChamelli RobinPas encore d'évaluation
- Case Study NCPDocument4 pagesCase Study NCPKelly OstolPas encore d'évaluation
- Situation 1Document18 pagesSituation 1Maler De VeraPas encore d'évaluation
- Community Duty Problem SheetDocument7 pagesCommunity Duty Problem SheetReed Dela CruzPas encore d'évaluation
- Cite One Role of The Community To Health and ExplainDocument3 pagesCite One Role of The Community To Health and ExplainAbegyl Nicole FiguraPas encore d'évaluation
- HEALTH-TEACHING (Safety)Document3 pagesHEALTH-TEACHING (Safety)Asterlyn ConiendoPas encore d'évaluation
- Historical Backgroud of DOHDocument4 pagesHistorical Backgroud of DOHAna LuisaPas encore d'évaluation
- Jerson Jeck AlcidoDocument5 pagesJerson Jeck AlcidoJerson Jeck Salumanda AlcidoPas encore d'évaluation
- Nursing Process in Drug TherapyDocument32 pagesNursing Process in Drug TherapyChasePas encore d'évaluation
- Nursing Diagnosis Cues Rank Justification According To ABC or Maslow'sDocument3 pagesNursing Diagnosis Cues Rank Justification According To ABC or Maslow'sShaina MillanPas encore d'évaluation
- Vega CHDPDocument5 pagesVega CHDPAlexandria P. OrcajadaPas encore d'évaluation
- Health Care Delivery System & COPARDocument52 pagesHealth Care Delivery System & COPARDharylle Cariño100% (1)
- SAS 7 - Abapo, Aquea B.Document3 pagesSAS 7 - Abapo, Aquea B.Aquea Bernardo AbapoPas encore d'évaluation
- Week 8 - Activity (Case Scenario)Document7 pagesWeek 8 - Activity (Case Scenario)Jollan Marie BuenvenidaPas encore d'évaluation
- Lonzaga Assessment PDFDocument7 pagesLonzaga Assessment PDFNiño Naryana Luke PanchoPas encore d'évaluation
- PointersDocument49 pagesPointersStephanie Villanueva AdvinculaPas encore d'évaluation
- Ranking and Scoring of Health ProblemsDocument2 pagesRanking and Scoring of Health ProblemsMonmon BagarinaoPas encore d'évaluation
- Orientation On Community Health - Doh Programs & ServicesDocument11 pagesOrientation On Community Health - Doh Programs & ServicesAudrey Beatrice ReyesPas encore d'évaluation
- SAS Session 4 Research 1Document6 pagesSAS Session 4 Research 1Leaflor Ann ManghihilotPas encore d'évaluation
- Nursing Care Plan Format Name: - Medical Diagnosis: Tetanus DateDocument2 pagesNursing Care Plan Format Name: - Medical Diagnosis: Tetanus DateSheryl Ann Barit PedinesPas encore d'évaluation
- Nur 154 P1Document16 pagesNur 154 P1Naomi VirtudazoPas encore d'évaluation
- FNCPDocument14 pagesFNCPhelloaPas encore d'évaluation
- Elements of FourMULA ONEDocument12 pagesElements of FourMULA ONEkassy yeonPas encore d'évaluation
- Community Health Nursing Review NotesDocument12 pagesCommunity Health Nursing Review NotesISICLE GTPas encore d'évaluation
- NCP Preeclampsia PDFDocument1 pageNCP Preeclampsia PDFTrixy Glaire TomasetePas encore d'évaluation
- CHN PTDocument2 pagesCHN PTYzobel Phoebe ParoanPas encore d'évaluation
- Midterm Period Course Task 2 Nurse Researcher Role.Document7 pagesMidterm Period Course Task 2 Nurse Researcher Role.Jhanina CapicioPas encore d'évaluation
- Nurses Assigned in Rural ServicesDocument3 pagesNurses Assigned in Rural ServicescubezeroPas encore d'évaluation
- Prioritization Scoring by MaglayaDocument3 pagesPrioritization Scoring by MaglayamaettPas encore d'évaluation
- FNCP ProperDocument3 pagesFNCP ProperSoniaMarieBalanayPas encore d'évaluation
- Water Source (Level 1) (Bacalla) : Criteria Score Weight Computation Actual Score JustificationDocument2 pagesWater Source (Level 1) (Bacalla) : Criteria Score Weight Computation Actual Score JustificationlovlyPas encore d'évaluation
- NCP Acabo Hypokalemia 1Document2 pagesNCP Acabo Hypokalemia 1Doneva Lyn MedinaPas encore d'évaluation
- Community AccomplishmentDocument2 pagesCommunity AccomplishmentRudy Mark ReyesPas encore d'évaluation
- Expanded Program Immunization: NCM 104: Community Health Nursing I: Individual and FamilyDocument25 pagesExpanded Program Immunization: NCM 104: Community Health Nursing I: Individual and FamilyRica machells DaydaPas encore d'évaluation
- Proper Excreta Disposal, Food Safety Sanitation-Video LecDocument15 pagesProper Excreta Disposal, Food Safety Sanitation-Video LecEden LacsonPas encore d'évaluation
- NCM 119 Assignment Galutan Kimberly Erika FDocument5 pagesNCM 119 Assignment Galutan Kimberly Erika Faaron tabernaPas encore d'évaluation
- Sample Scale Ranking en FNCPDocument7 pagesSample Scale Ranking en FNCPABDULRAHMAN MISHARI AL-THABITPas encore d'évaluation
- Respi SystemDocument65 pagesRespi Systemapi-373599567% (3)
- SDL3Document2 pagesSDL3Margaux BaynosaPas encore d'évaluation
- Propranolol, Prophylactic Warfarin, Low Molecular Weight Heparin (LMWH), Furosemide, AntibioticsDocument8 pagesPropranolol, Prophylactic Warfarin, Low Molecular Weight Heparin (LMWH), Furosemide, AntibioticsArlyn MarcelinoPas encore d'évaluation
- Personal-Soc Interpretation: Tower of 4 CubesDocument15 pagesPersonal-Soc Interpretation: Tower of 4 CubesteuuuuPas encore d'évaluation
- COMMUNITY-MANUSCRIPT SampleDocument84 pagesCOMMUNITY-MANUSCRIPT SampleCA SavagePas encore d'évaluation
- Module 5 Hiv Aids NRG 301Document17 pagesModule 5 Hiv Aids NRG 301EMMY FLOR VALMORIAPas encore d'évaluation
- Community Health NursingDocument105 pagesCommunity Health NursingKBDPas encore d'évaluation
- TB Action Plan: Results of Discussion and AgreementDocument10 pagesTB Action Plan: Results of Discussion and AgreementSimon S. KledenPas encore d'évaluation
- CMCQDocument31 pagesCMCQJim Christian EllaserPas encore d'évaluation
- Community Dentistry Ii: Planning - It Is A Decision About A Course of ActionDocument8 pagesCommunity Dentistry Ii: Planning - It Is A Decision About A Course of ActionMark Anthony C. MalubagPas encore d'évaluation
- Mod2 - Ch5 - Introduction To Health ProgramsDocument6 pagesMod2 - Ch5 - Introduction To Health ProgramsWilujeng FajriyatilPas encore d'évaluation
- Community Health ProgramDocument43 pagesCommunity Health ProgramBsoom .iPas encore d'évaluation
- 2011-0021 22 Research MethodologyDocument43 pages2011-0021 22 Research MethodologymarcamillePas encore d'évaluation
- Ecotourism in Palawan: A Case Study: Chapter Twenty-OneDocument5 pagesEcotourism in Palawan: A Case Study: Chapter Twenty-OnemarcamillePas encore d'évaluation
- Best Ref Action Research For TeachersDocument30 pagesBest Ref Action Research For TeachersmarcamillePas encore d'évaluation
- 40S Be 0889Document54 pages40S Be 0889Ankit SinghPas encore d'évaluation
- 2011-0021 22 Research MethodologyDocument18 pages2011-0021 22 Research Methodologyahmedbalo100% (1)
- Cooperative LearningDocument93 pagesCooperative LearningmarcamillePas encore d'évaluation
- Policy Guidelines in Daily LessonsDocument62 pagesPolicy Guidelines in Daily LessonsmarcamillePas encore d'évaluation
- Action ResearchDocument43 pagesAction ResearchAmirah Izzati Nor Azam100% (2)
- SHS Core - Understanding Culture, Society and Politics CGDocument1 pageSHS Core - Understanding Culture, Society and Politics CGmarcamillePas encore d'évaluation
- Disaster UnescoDocument58 pagesDisaster UnescomarcamillePas encore d'évaluation
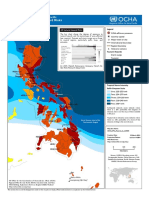
- Phil Natural Hazard MapDocument25 pagesPhil Natural Hazard MapmarcamillePas encore d'évaluation
- SHS Understanding Culture, Society and Politics CGDocument8 pagesSHS Understanding Culture, Society and Politics CGLloyl Yosores Montero67% (24)
- Phil Natural Hazard Map PDFDocument1 pagePhil Natural Hazard Map PDFmarcamillePas encore d'évaluation
- Basic Nursing: Foundations of Skills and Concepts: Holistic CareDocument14 pagesBasic Nursing: Foundations of Skills and Concepts: Holistic CareAnggi KusumaPas encore d'évaluation
- Cci11072017 0003Document1 pageCci11072017 0003marcamillePas encore d'évaluation
- TittleDocument1 pageTittlemarcamillePas encore d'évaluation
- Cancer (PCS) 03Document50 pagesCancer (PCS) 03marcamillePas encore d'évaluation
- Things To BringDocument1 pageThings To BringmarcamillePas encore d'évaluation
- SHS Core - Oral Communication CGDocument7 pagesSHS Core - Oral Communication CGEstela Benegildo67% (3)
- Diarrhea (PSG) 03Document23 pagesDiarrhea (PSG) 03Princez_Perez_9554Pas encore d'évaluation
- Department of Nursing Evaluation Tool - Clinical Practice (Level 2 To 4)Document2 pagesDepartment of Nursing Evaluation Tool - Clinical Practice (Level 2 To 4)marcamillePas encore d'évaluation
- Action ResearchDocument43 pagesAction ResearchAmirah Izzati Nor Azam100% (2)
- 1st FHSIS Indicator and FormulaDocument2 pages1st FHSIS Indicator and Formulamarcamille100% (2)
- Oral Communication in Context TG For SHSDocument100 pagesOral Communication in Context TG For SHSJolly Mar Tabbaban Mangilaya80% (5)
- SHS Applied - Research 2 CG PDFDocument6 pagesSHS Applied - Research 2 CG PDFJakie UbinaPas encore d'évaluation
- Proposal Water Vendo MachineDocument10 pagesProposal Water Vendo Machinemarcamille100% (4)
- Subsidiary Practical ResearchDocument3 pagesSubsidiary Practical ResearchmarcamillePas encore d'évaluation
- Bloom's TaxonomyDocument24 pagesBloom's TaxonomymarcamillePas encore d'évaluation
- Analyzing SynthesizingDocument2 pagesAnalyzing SynthesizingMaria SantosPas encore d'évaluation
- Chapter 7 - Managing Project SchedulesDocument10 pagesChapter 7 - Managing Project Schedulesfadi warthPas encore d'évaluation
- Defining Strategic ManagementDocument5 pagesDefining Strategic Managementnabilana26Pas encore d'évaluation
- 2017 The Application Guide For The Deming Prize2017.en - EsDocument74 pages2017 The Application Guide For The Deming Prize2017.en - EsCarlos DianderasPas encore d'évaluation
- Latrobe Street Saleyards Background AnalysisDocument26 pagesLatrobe Street Saleyards Background Analysisjolyon AttwoollPas encore d'évaluation
- Griffin - ch06 Planning and Decison MakingDocument29 pagesGriffin - ch06 Planning and Decison MakingMd HimelPas encore d'évaluation
- SwapnoDocument25 pagesSwapnoMd Shah Ahsan Leon0% (3)
- Enterprise Architecture Planning in Developing A P PDFDocument9 pagesEnterprise Architecture Planning in Developing A P PDFmarlon dungoPas encore d'évaluation
- Tourism Planning and Policy: Indira Gandhi National Open University School of Tourism Hospitality Service ManagementDocument56 pagesTourism Planning and Policy: Indira Gandhi National Open University School of Tourism Hospitality Service ManagementFaizy_5starPas encore d'évaluation
- The Coaching Habit: Say Less, Ask More & Change the Way You Lead ForeverD'EverandThe Coaching Habit: Say Less, Ask More & Change the Way You Lead ForeverÉvaluation : 4.5 sur 5 étoiles4.5/5 (186)
- The First Minute: How to start conversations that get resultsD'EverandThe First Minute: How to start conversations that get resultsÉvaluation : 4.5 sur 5 étoiles4.5/5 (57)
- The 7 Habits of Highly Effective PeopleD'EverandThe 7 Habits of Highly Effective PeopleÉvaluation : 4 sur 5 étoiles4/5 (2565)
- Scaling Up: How a Few Companies Make It...and Why the Rest Don't, Rockefeller Habits 2.0D'EverandScaling Up: How a Few Companies Make It...and Why the Rest Don't, Rockefeller Habits 2.0Évaluation : 5 sur 5 étoiles5/5 (1)
- How to Lead: Wisdom from the World's Greatest CEOs, Founders, and Game ChangersD'EverandHow to Lead: Wisdom from the World's Greatest CEOs, Founders, and Game ChangersÉvaluation : 4.5 sur 5 étoiles4.5/5 (95)
- Summary of Noah Kagan's Million Dollar WeekendD'EverandSummary of Noah Kagan's Million Dollar WeekendÉvaluation : 5 sur 5 étoiles5/5 (1)
- How to Talk to Anyone at Work: 72 Little Tricks for Big Success Communicating on the JobD'EverandHow to Talk to Anyone at Work: 72 Little Tricks for Big Success Communicating on the JobÉvaluation : 4.5 sur 5 étoiles4.5/5 (36)
- Only the Paranoid Survive: How to Exploit the Crisis Points That Challenge Every CompanyD'EverandOnly the Paranoid Survive: How to Exploit the Crisis Points That Challenge Every CompanyÉvaluation : 3.5 sur 5 étoiles3.5/5 (122)
- 25 Ways to Win with People: How to Make Others Feel Like a Million BucksD'Everand25 Ways to Win with People: How to Make Others Feel Like a Million BucksÉvaluation : 5 sur 5 étoiles5/5 (36)
- Spark: How to Lead Yourself and Others to Greater SuccessD'EverandSpark: How to Lead Yourself and Others to Greater SuccessÉvaluation : 4.5 sur 5 étoiles4.5/5 (132)
- Transformed: Moving to the Product Operating ModelD'EverandTransformed: Moving to the Product Operating ModelÉvaluation : 4 sur 5 étoiles4/5 (1)
- The 7 Habits of Highly Effective People: 30th Anniversary EditionD'EverandThe 7 Habits of Highly Effective People: 30th Anniversary EditionÉvaluation : 5 sur 5 étoiles5/5 (337)
- Coach the Person, Not the Problem: A Guide to Using Reflective InquiryD'EverandCoach the Person, Not the Problem: A Guide to Using Reflective InquiryÉvaluation : 5 sur 5 étoiles5/5 (64)
- Work the System: The Simple Mechanics of Making More and Working Less (4th Edition)D'EverandWork the System: The Simple Mechanics of Making More and Working Less (4th Edition)Évaluation : 4.5 sur 5 étoiles4.5/5 (23)
- Billion Dollar Lessons: What You Can Learn from the Most Inexcusable Business Failures of the Last Twenty-five YearsD'EverandBillion Dollar Lessons: What You Can Learn from the Most Inexcusable Business Failures of the Last Twenty-five YearsÉvaluation : 4.5 sur 5 étoiles4.5/5 (52)
- Radical Candor by Kim Scott - Book Summary: Be A Kickass Boss Without Losing Your HumanityD'EverandRadical Candor by Kim Scott - Book Summary: Be A Kickass Boss Without Losing Your HumanityÉvaluation : 4.5 sur 5 étoiles4.5/5 (40)
- The 12 Week Year: Get More Done in 12 Weeks than Others Do in 12 MonthsD'EverandThe 12 Week Year: Get More Done in 12 Weeks than Others Do in 12 MonthsÉvaluation : 4.5 sur 5 étoiles4.5/5 (411)
- Transformed: Moving to the Product Operating ModelD'EverandTransformed: Moving to the Product Operating ModelÉvaluation : 4 sur 5 étoiles4/5 (1)
- The Introverted Leader: Building on Your Quiet StrengthD'EverandThe Introverted Leader: Building on Your Quiet StrengthÉvaluation : 4.5 sur 5 étoiles4.5/5 (35)
- The Power of People Skills: How to Eliminate 90% of Your HR Problems and Dramatically Increase Team and Company Morale and PerformanceD'EverandThe Power of People Skills: How to Eliminate 90% of Your HR Problems and Dramatically Increase Team and Company Morale and PerformanceÉvaluation : 5 sur 5 étoiles5/5 (22)
- Work Stronger: Habits for More Energy, Less Stress, and Higher Performance at WorkD'EverandWork Stronger: Habits for More Energy, Less Stress, and Higher Performance at WorkÉvaluation : 4.5 sur 5 étoiles4.5/5 (12)
- The Effective Executive: The Definitive Guide to Getting the Right Things DoneD'EverandThe Effective Executive: The Definitive Guide to Getting the Right Things DoneÉvaluation : 4.5 sur 5 étoiles4.5/5 (469)
- The E-Myth Revisited: Why Most Small Businesses Don't Work andD'EverandThe E-Myth Revisited: Why Most Small Businesses Don't Work andÉvaluation : 4.5 sur 5 étoiles4.5/5 (709)
- Sustainability Management: Global Perspectives on Concepts, Instruments, and StakeholdersD'EverandSustainability Management: Global Perspectives on Concepts, Instruments, and StakeholdersÉvaluation : 5 sur 5 étoiles5/5 (1)
- Management Mess to Leadership Success: 30 Challenges to Become the Leader You Would FollowD'EverandManagement Mess to Leadership Success: 30 Challenges to Become the Leader You Would FollowÉvaluation : 4.5 sur 5 étoiles4.5/5 (27)
- The Little Big Things: 163 Ways to Pursue ExcellenceD'EverandThe Little Big Things: 163 Ways to Pursue ExcellencePas encore d'évaluation
- 7 Principles of Transformational Leadership: Create a Mindset of Passion, Innovation, and GrowthD'Everand7 Principles of Transformational Leadership: Create a Mindset of Passion, Innovation, and GrowthÉvaluation : 5 sur 5 étoiles5/5 (52)