Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- UploadFiles - Download - eResin-PLA Pro Recommended Settings For PrinterDocument6 pagesUploadFiles - Download - eResin-PLA Pro Recommended Settings For PrinterDesrainy InhardiniPas encore d'évaluation
- Ivanov 2011Document2 pagesIvanov 2011Desrainy InhardiniPas encore d'évaluation
- Haug 1999Document7 pagesHaug 1999Desrainy InhardiniPas encore d'évaluation
- Merritt 2005Document8 pagesMerritt 2005Desrainy InhardiniPas encore d'évaluation
- Marcus 2017Document17 pagesMarcus 2017Desrainy InhardiniPas encore d'évaluation
- Fullpapers DPDocument10 pagesFullpapers DPDesrainy InhardiniPas encore d'évaluation
- Admin, EDITED - 8 NASAL AESTHETIC EVALUATION FOLLOWING PRE-SURGICAL NASO-ALVEOLAR MOLDINGDocument9 pagesAdmin, EDITED - 8 NASAL AESTHETIC EVALUATION FOLLOWING PRE-SURGICAL NASO-ALVEOLAR MOLDINGArnPas encore d'évaluation
- Primary Correction of The Unilateral Cleft Lip Nasal Deformity: Achieving The ExcellenceDocument6 pagesPrimary Correction of The Unilateral Cleft Lip Nasal Deformity: Achieving The ExcellenceDesrainy InhardiniPas encore d'évaluation
- Ivanov 2011Document2 pagesIvanov 2011Desrainy InhardiniPas encore d'évaluation
- Facial Reconstruction Using Polypropylene Mesh After Resection of Maxillary Ossifying FibromaDocument5 pagesFacial Reconstruction Using Polypropylene Mesh After Resection of Maxillary Ossifying FibromaDesrainy InhardiniPas encore d'évaluation
- Fullpapers DPDocument10 pagesFullpapers DPDesrainy InhardiniPas encore d'évaluation
- Face SubunitsDocument5 pagesFace SubunitsDeevish N DinakarPas encore d'évaluation
- Late-Onset Inflammation in Asian Rhinoplasty Using Alloplastic ImplantsDocument9 pagesLate-Onset Inflammation in Asian Rhinoplasty Using Alloplastic ImplantsDesrainy InhardiniPas encore d'évaluation
- Late-Onset Inflammation in Asian Rhinoplasty Using Alloplastic ImplantsDocument9 pagesLate-Onset Inflammation in Asian Rhinoplasty Using Alloplastic ImplantsDesrainy InhardiniPas encore d'évaluation
- Emergency Management of Severe Burns Manual: February 2012Document3 pagesEmergency Management of Severe Burns Manual: February 2012TommysPas encore d'évaluation
- Physical Examination of The Hand: Cme Information and DisclosuresDocument11 pagesPhysical Examination of The Hand: Cme Information and DisclosuresDesrainy InhardiniPas encore d'évaluation
- GCS PDFDocument1 pageGCS PDFFrincia100% (1)
- Values of A Patient and Observer Scar Assessment SDocument9 pagesValues of A Patient and Observer Scar Assessment SDesrainy InhardiniPas encore d'évaluation
- Pediatrics 2014 Li E917 22Document8 pagesPediatrics 2014 Li E917 22Desrainy InhardiniPas encore d'évaluation
- Pediatrics 2014 Blyth E1218 25Document10 pagesPediatrics 2014 Blyth E1218 25Desrainy InhardiniPas encore d'évaluation
- Pediatrics 2014 Leshem 15 23Document11 pagesPediatrics 2014 Leshem 15 23Desrainy InhardiniPas encore d'évaluation
- Normal ValuesDocument6 pagesNormal ValuesMc Crister SilangPas encore d'évaluation
- Pediatrics 2014 Hambidge E1492 9Document10 pagesPediatrics 2014 Hambidge E1492 9Desrainy InhardiniPas encore d'évaluation
- Journal ReadingDocument14 pagesJournal ReadingDesrainy InhardiniPas encore d'évaluation
- Normal ValuesDocument6 pagesNormal ValuesMc Crister SilangPas encore d'évaluation
- Pediatrics 2014 Queen E23 9Document10 pagesPediatrics 2014 Queen E23 9Desrainy InhardiniPas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Stuck Up!!! - Case Report of A Rectal Foreign BodyDocument6 pagesStuck Up!!! - Case Report of A Rectal Foreign BodyIJAR JOURNALPas encore d'évaluation
- Kopkash 2018Document6 pagesKopkash 2018Yefry Onil Santana MartePas encore d'évaluation
- Ectopic PregnancyDocument10 pagesEctopic PregnancyRegine AldamarPas encore d'évaluation
- Organizing Neonatal CareDocument17 pagesOrganizing Neonatal CareManisha ThakurPas encore d'évaluation
- Case Study Presented by Group 22 BSN 206: In-Depth View On CholecystectomyDocument46 pagesCase Study Presented by Group 22 BSN 206: In-Depth View On CholecystectomyAjiMary M. DomingoPas encore d'évaluation
- Procedure Checklist Chapter 23: Using A Volume-Control Administration Set (E.g., Buretrol, Volutrol, Soluset)Document2 pagesProcedure Checklist Chapter 23: Using A Volume-Control Administration Set (E.g., Buretrol, Volutrol, Soluset)jthsPas encore d'évaluation
- Presentation On Care of Critically Ill PatientDocument9 pagesPresentation On Care of Critically Ill Patientanamika sharmaPas encore d'évaluation
- Modes of VentilatorDocument10 pagesModes of VentilatorSatya Biomed100% (1)
- Labeled ItDocument50 pagesLabeled ItKaloy KamaoPas encore d'évaluation
- Circulatory System ExplainedDocument3 pagesCirculatory System ExplainedJjongPas encore d'évaluation
- Comparison of A New Flap Design With The Routinely Used Triangular Flap Design in Third Molar SurgeryDocument8 pagesComparison of A New Flap Design With The Routinely Used Triangular Flap Design in Third Molar SurgeryJean Carlos Barbosa FerreiraPas encore d'évaluation
- Nelson2014 Hialuronidase em HematomasDocument3 pagesNelson2014 Hialuronidase em HematomasPaula AzevedoPas encore d'évaluation
- Clinical EndodonticsDocument30 pagesClinical EndodonticsJemmy WendyPas encore d'évaluation
- Basic Life Support: Practice Test QuestionsDocument6 pagesBasic Life Support: Practice Test QuestionsDay Moreno100% (3)
- Anatomy, Abdomen and Pelvis, Kidneys: Statpearls (Internet) - Treasure Island (FL) : Statpearls Publishing 2022 JanDocument6 pagesAnatomy, Abdomen and Pelvis, Kidneys: Statpearls (Internet) - Treasure Island (FL) : Statpearls Publishing 2022 Janvenus ohPas encore d'évaluation
- Managing - Patients - With - Severe - Traumatic - Brain WITH HIGHLIGHTSDocument8 pagesManaging - Patients - With - Severe - Traumatic - Brain WITH HIGHLIGHTSTre OfficialPas encore d'évaluation
- NeonatalresuscitationDocument67 pagesNeonatalresuscitationfidaPas encore d'évaluation
- Atlas of Pelvic Anatomy and Gynecologic Surgery (Histerectomia)Document34 pagesAtlas of Pelvic Anatomy and Gynecologic Surgery (Histerectomia)Jose Augusto Antonio Alves Flor0% (1)
- Artifacts in HistopathologyDocument8 pagesArtifacts in Histopathologysyed ahmedPas encore d'évaluation
- Periodontal Regeneration in Vital and Nonvital Teeth - A Clinical StudyDocument28 pagesPeriodontal Regeneration in Vital and Nonvital Teeth - A Clinical Studyneetika guptaPas encore d'évaluation
- Osteology and Gluteal Region TransDocument18 pagesOsteology and Gluteal Region Transchynne ongPas encore d'évaluation
- ACFrOgDACnKE0rUjf42HXaSb36Wbju Urd7BPPqmTBRXMMFtZ91-fOr1fErSfh6BzXghJFKNYiKG5H-y3ET76l8IkKipRRxFa4B6gSp0OP6njH7C 5ulv8f C1cL DaDocument209 pagesACFrOgDACnKE0rUjf42HXaSb36Wbju Urd7BPPqmTBRXMMFtZ91-fOr1fErSfh6BzXghJFKNYiKG5H-y3ET76l8IkKipRRxFa4B6gSp0OP6njH7C 5ulv8f C1cL Dajelena_stankovic_34Pas encore d'évaluation
- A Case Study On The Use of Technology in Medicine: Robotic SurgeryDocument11 pagesA Case Study On The Use of Technology in Medicine: Robotic SurgeryJohn Mark EmataPas encore d'évaluation
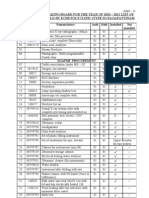
- Annual Stock Taking Board For The Year of 2010 - 2011 List of Maj Med Eqpt-Held by Echs Polyclinic (Type-D) NagapattinamDocument17 pagesAnnual Stock Taking Board For The Year of 2010 - 2011 List of Maj Med Eqpt-Held by Echs Polyclinic (Type-D) NagapattinamechsngtPas encore d'évaluation
- Instrumentation and Techniques in Equine Fracture Fixation: Joerg Auer, OMV, MS and Jeffrey P Watkins, DVM, MSDocument20 pagesInstrumentation and Techniques in Equine Fracture Fixation: Joerg Auer, OMV, MS and Jeffrey P Watkins, DVM, MSSergio Nieves MoranPas encore d'évaluation
- Gore EndoprotesesDocument4 pagesGore EndoprotesesLivio NakanoPas encore d'évaluation
- Meniscal Root Repair Using A Two-Tunnel Technique: Smith&nephewDocument16 pagesMeniscal Root Repair Using A Two-Tunnel Technique: Smith&nephewAlejandro RodriguezPas encore d'évaluation
- COPD and asthma diagnostic tests and treatment guidelinesDocument40 pagesCOPD and asthma diagnostic tests and treatment guidelinesDiaconu AndreeaPas encore d'évaluation
- Mammography and Breast Localization For The InterventionalistDocument6 pagesMammography and Breast Localization For The InterventionalistrasminojPas encore d'évaluation
- Pcs Question 1Document21 pagesPcs Question 1Azra MuzafarPas encore d'évaluation