Vous aimerez peut-être aussi
- Ijm 11 488Document8 pagesIjm 11 488farida santiPas encore d'évaluation
- Pharmaceutical Sciences: Finding of Organisms Causing Bacteriuria in Pregnant WomenDocument4 pagesPharmaceutical Sciences: Finding of Organisms Causing Bacteriuria in Pregnant WomeniajpsPas encore d'évaluation
- Study of Relationship Between Anemia and Urinary Tract Infection in Pregnant WomenDocument5 pagesStudy of Relationship Between Anemia and Urinary Tract Infection in Pregnant WomenIvana ThiodoraPas encore d'évaluation
- RCOG Review Urinary Tract InfectionDocument7 pagesRCOG Review Urinary Tract InfectionAji NuswantoroPas encore d'évaluation
- Asymp Bact in Urin Kath AncDocument4 pagesAsymp Bact in Urin Kath AncDERRICK AAGYEREYIR SAANUMEPas encore d'évaluation
- Molecular Detection of Microbial Colonization in Cervical MucusDocument9 pagesMolecular Detection of Microbial Colonization in Cervical MucusHAVIZ YUADPas encore d'évaluation
- Jurnal ObgynDocument10 pagesJurnal ObgynTiffany Rachma PutriPas encore d'évaluation
- Bacteria Profile Associated With Bacteriuria in Pregnancy at The Yaounde University Teaching Hospital (CHUY)Document12 pagesBacteria Profile Associated With Bacteriuria in Pregnancy at The Yaounde University Teaching Hospital (CHUY)International Journal of Innovative Science and Research TechnologyPas encore d'évaluation
- Mojbm 03 00082Document5 pagesMojbm 03 00082Sohrab RohanePas encore d'évaluation
- Virulence and Resistance Characterization of StaphDocument14 pagesVirulence and Resistance Characterization of StaphSri PrihandaniPas encore d'évaluation
- Jurnal AborsiDocument6 pagesJurnal Aborsimakiyatul madaniaPas encore d'évaluation
- 1756 0500 5 197Document7 pages1756 0500 5 197El tren del MamePas encore d'évaluation
- Aborto Septico 2020Document5 pagesAborto Septico 2020Adrian Pardo VillegasPas encore d'évaluation
- Prevalence of Bacterial Vaginosis in Pregnant Women in Maiduguri, North-Eastern NigeriaDocument10 pagesPrevalence of Bacterial Vaginosis in Pregnant Women in Maiduguri, North-Eastern NigeriaRetno Agusty WulandariPas encore d'évaluation
- Gynaecology: Dr. Chintamani Mohanta Dr. Kumudini PradhanDocument7 pagesGynaecology: Dr. Chintamani Mohanta Dr. Kumudini PradhanPrima Hari PratamaPas encore d'évaluation
- Urogenital Infections - A Cause of Pre Term LaborDocument4 pagesUrogenital Infections - A Cause of Pre Term LaborPangalanitaPas encore d'évaluation
- JCDR 11 DC18Document5 pagesJCDR 11 DC18Putri YunandaPas encore d'évaluation
- Telaah Jurnal Annisa Nabilla 11120222180Document20 pagesTelaah Jurnal Annisa Nabilla 11120222180annisa nabilaPas encore d'évaluation
- Manifestasi Klinis 2Document9 pagesManifestasi Klinis 2avely NathessaPas encore d'évaluation
- Klebsiella Pneumoniae Isolated From Urine ofDocument9 pagesKlebsiella Pneumoniae Isolated From Urine ofInternational Journal of Innovative Science and Research TechnologyPas encore d'évaluation
- UntitledDocument13 pagesUntitledAngela PunayPas encore d'évaluation
- 1 1 71Document8 pages1 1 71Medical JournalPas encore d'évaluation
- Clinical and Microbiological Features of Bartholin's Gland Abscess in Pregnant and Non-Pregnant WomenDocument7 pagesClinical and Microbiological Features of Bartholin's Gland Abscess in Pregnant and Non-Pregnant WomenHand SanitizerPas encore d'évaluation
- 503 PDFDocument5 pages503 PDFAlda CarlynePas encore d'évaluation
- Ni Hms 731282Document54 pagesNi Hms 731282ichaPas encore d'évaluation
- 7225-Article Text For Production-20461-1-10-20231016Document12 pages7225-Article Text For Production-20461-1-10-20231016grovy90Pas encore d'évaluation
- Paper On Bact VaginosisDocument16 pagesPaper On Bact VaginosisWael GaberPas encore d'évaluation
- European Journal of Obstetrics & Gynecology and Reproductive BiologyDocument4 pagesEuropean Journal of Obstetrics & Gynecology and Reproductive BiologyThomas Regina PutraPas encore d'évaluation
- Infestation of Endometrium by Mycobacterium Tuberculosis Bacilli-Cause of Reproductive FailureDocument10 pagesInfestation of Endometrium by Mycobacterium Tuberculosis Bacilli-Cause of Reproductive FailureMathivanan AnbazhaganPas encore d'évaluation
- AldunateDocument23 pagesAldunateFelipe MPas encore d'évaluation
- Chen 2015Document3 pagesChen 2015Néfer TitiPas encore d'évaluation
- 6 of Vaginal DischargeDocument4 pages6 of Vaginal DischargePanjul NugrohoPas encore d'évaluation
- Pustotina (2019) 19 - Effects of Antibiotictherapy in Women With The Amniotic FluidsDocument14 pagesPustotina (2019) 19 - Effects of Antibiotictherapy in Women With The Amniotic FluidsRodrigo MelloPas encore d'évaluation
- Ijmmtd 24 171-174Document5 pagesIjmmtd 24 171-174prabaPas encore d'évaluation
- PresusDocument6 pagesPresusFrishia DidaPas encore d'évaluation
- Jurnal BVDocument3 pagesJurnal BVEnvhy WinaPas encore d'évaluation
- Prevention of Urinary Tract Infection in Six Spinal Cord Injured Pregnant Women Who Gave Birth To Seven Children Under A Weekly Oral Cyclic Antibiotic Program PDFDocument4 pagesPrevention of Urinary Tract Infection in Six Spinal Cord Injured Pregnant Women Who Gave Birth To Seven Children Under A Weekly Oral Cyclic Antibiotic Program PDFMaría Alejandra López AriasPas encore d'évaluation
- Impact of Bacterial Vaginosis On Perineal Tears During Delivery: A Prospective Cohort StudyDocument9 pagesImpact of Bacterial Vaginosis On Perineal Tears During Delivery: A Prospective Cohort Studysiti hazard aldinaPas encore d'évaluation
- Female Urinary Tract Infections in Clinical PracticeD'EverandFemale Urinary Tract Infections in Clinical PracticeBob YangPas encore d'évaluation
- Vaginal Microbiota E150-1Document56 pagesVaginal Microbiota E150-1shomowwPas encore d'évaluation
- Urinary Tract Infections During PregnancyDocument8 pagesUrinary Tract Infections During PregnancyGloria SaldivarPas encore d'évaluation
- Keywords: Group B Streptococcus, Colonization, Prevalence, Factors Associated, AntibioticDocument15 pagesKeywords: Group B Streptococcus, Colonization, Prevalence, Factors Associated, AntibioticKIU PUBLICATION AND EXTENSIONPas encore d'évaluation
- Composition of Vaginal Microbiota and Their Antibiotic Susceptibility in Symptomatic WomenDocument6 pagesComposition of Vaginal Microbiota and Their Antibiotic Susceptibility in Symptomatic WomenAmirah MohdPas encore d'évaluation
- Tijjani, R. J., Yahaya, O. and Inabo, H. I.: UJMR, Volume 5 Number 1, June, 2020, PP 1 - 8Document8 pagesTijjani, R. J., Yahaya, O. and Inabo, H. I.: UJMR, Volume 5 Number 1, June, 2020, PP 1 - 8UMYU Journal of Microbiology Research (UJMR)Pas encore d'évaluation
- Intestinal Colonization With Multidrug-Resistant Enterobacteriaceae in A Healthy Adult PopulationDocument8 pagesIntestinal Colonization With Multidrug-Resistant Enterobacteriaceae in A Healthy Adult PopulationOpenaccess Research paperPas encore d'évaluation
- 1 SMDocument14 pages1 SMBerryEkaPardaBancinPas encore d'évaluation
- Bacteriological Profile and Antibiogram of Urinary Tract Infections in A Tertiary Care HospitalDocument5 pagesBacteriological Profile and Antibiogram of Urinary Tract Infections in A Tertiary Care HospitalOpenaccess Research paperPas encore d'évaluation
- Pregnant Women in West GojjamDocument10 pagesPregnant Women in West Gojjambluish oceanPas encore d'évaluation
- Management of Disease and Disorders by Prebiotics and Probiotic Therapy: Probiotics in Bacterial VaginosisDocument9 pagesManagement of Disease and Disorders by Prebiotics and Probiotic Therapy: Probiotics in Bacterial Vaginosissiska tiaraPas encore d'évaluation
- Evaluation of The Bacterial Agents Associated With PID Among Women of Reproductive Age at Kampala International University Teaching Hospital.Document12 pagesEvaluation of The Bacterial Agents Associated With PID Among Women of Reproductive Age at Kampala International University Teaching Hospital.KIU PUBLICATION AND EXTENSIONPas encore d'évaluation
- Rfra MoaDocument10 pagesRfra MoaDimes Atika PermanasariPas encore d'évaluation
- Small Animal - Nephrology and UrologyDocument3 pagesSmall Animal - Nephrology and UrologyNana juniartiPas encore d'évaluation
- Clinical Therapy of UTI in Children Under The Age of Five Varies WidelyDocument21 pagesClinical Therapy of UTI in Children Under The Age of Five Varies WidelyInternational Journal of Innovative Science and Research TechnologyPas encore d'évaluation
- Bacteria Found in UrineDocument7 pagesBacteria Found in UrineAria DomingoPas encore d'évaluation
- The Urinary Microbiome in Postmenopausal Women With Recurrent Urinary Tract InfectionsDocument19 pagesThe Urinary Microbiome in Postmenopausal Women With Recurrent Urinary Tract InfectionsMARTINA MARIA INSUA CASTROPas encore d'évaluation
- Comparison of PCR, Culturing and Pap Smear Microscopy For Accurate Diagnosis of Genital ActinomycesDocument7 pagesComparison of PCR, Culturing and Pap Smear Microscopy For Accurate Diagnosis of Genital Actinomycestitaamalinda28Pas encore d'évaluation
- Probiotics For Prevention of Recurrent Vulvovaginal Candidiasis: A ReviewDocument7 pagesProbiotics For Prevention of Recurrent Vulvovaginal Candidiasis: A ReviewMURNI RAHAYUPas encore d'évaluation
- Diagnosis and Management of Ectopic Pregnancy-A Basic View Through LiteratureDocument2 pagesDiagnosis and Management of Ectopic Pregnancy-A Basic View Through LiteraturefprasasyaaPas encore d'évaluation
- Bacteriuria AsintomaticaDocument12 pagesBacteriuria AsintomaticaJuan Sebastian PedrazaPas encore d'évaluation
- Emerging Trends of Extended Spectrum Beta - Lactamase and Metallo-Beta Lactamase Escherichia Coli Strains Among Pregnant Women in Mile 4 Hospital, Abakaliki Implications For AntenataDocument10 pagesEmerging Trends of Extended Spectrum Beta - Lactamase and Metallo-Beta Lactamase Escherichia Coli Strains Among Pregnant Women in Mile 4 Hospital, Abakaliki Implications For AntenataKIU PUBLICATION AND EXTENSIONPas encore d'évaluation
- PatomekanismeDocument18 pagesPatomekanismeEdwin Pasha Jr.Pas encore d'évaluation
- Jurnal 3Document9 pagesJurnal 3Edwin Pasha Jr.Pas encore d'évaluation
- Jurnal 2Document16 pagesJurnal 2Edwin Pasha Jr.Pas encore d'évaluation
- Daftar Pustaka PashaDocument1 pageDaftar Pustaka PashaEdwin Pasha Jr.Pas encore d'évaluation
- Case Report: A Case of Drug Reaction With Eosinophilia and Systemic SymptomsDocument5 pagesCase Report: A Case of Drug Reaction With Eosinophilia and Systemic SymptomsEdwin Pasha Jr.Pas encore d'évaluation
- GaulDocument11 pagesGaulEdwin Pasha Jr.Pas encore d'évaluation
- Self Regulatory Games For ChildrenDocument5 pagesSelf Regulatory Games For ChildrenKIP-HIDRAULIKA MPas encore d'évaluation
- Art App Finals OutputDocument3 pagesArt App Finals OutputChariz Kate DungogPas encore d'évaluation
- M03 Study GuideDocument5 pagesM03 Study GuideMartina Vegel DavidsonPas encore d'évaluation
- How The Tortoise Got Its ScarsDocument3 pagesHow The Tortoise Got Its ScarsAngelenwPas encore d'évaluation
- Motion To Revoke Detention OrderDocument21 pagesMotion To Revoke Detention OrderStephen LoiaconiPas encore d'évaluation
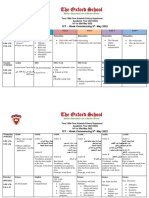
- Term 3 Mid-Term Assessment ScheduleDocument9 pagesTerm 3 Mid-Term Assessment ScheduleRabia MoeedPas encore d'évaluation
- Elasticity of Supply and Demand SessionDocument23 pagesElasticity of Supply and Demand SessionCharlizeK0% (1)
- Elasticity of Demand: Managerial EconomicsDocument41 pagesElasticity of Demand: Managerial EconomicsSomasundaram LakshminarasimhanPas encore d'évaluation
- Mba Final Project DaviDocument61 pagesMba Final Project DaviHarjagjeet singh0% (1)
- NarcissusDocument84 pagesNarcissusAlexandra Maria NeaguPas encore d'évaluation
- Voloxal TabletsDocument9 pagesVoloxal Tabletselcapitano vegetaPas encore d'évaluation
- Home DepotDocument13 pagesHome DepotTyfanie PetersenPas encore d'évaluation
- Chapter 14 Chemical EquilibriumDocument29 pagesChapter 14 Chemical EquilibriumlynloePas encore d'évaluation
- M 1.2 RMDocument16 pagesM 1.2 RMk thejeshPas encore d'évaluation
- BergsonDocument17 pagesBergsonAnonymous p3lyFYPas encore d'évaluation
- Theatre History TimelineDocument7 pagesTheatre History TimelineCzar Paulo Dabon100% (2)
- How To Reset AutoCAD To Defaults - AutoCAD 2019 - Autodesk Knowledge NetworkDocument11 pagesHow To Reset AutoCAD To Defaults - AutoCAD 2019 - Autodesk Knowledge NetworkZina MorPas encore d'évaluation
- Kutuzov A Life in War and Peace Alexander Mikaberidze 2 Full ChapterDocument67 pagesKutuzov A Life in War and Peace Alexander Mikaberidze 2 Full Chapterjanice.brooks978100% (6)
- Z Transform Part 1 PDFDocument16 pagesZ Transform Part 1 PDFAnanth SettyPas encore d'évaluation
- The Body Shop Marketing Plan AnalysisDocument18 pagesThe Body Shop Marketing Plan AnalysisHepita0% (1)
- Elements of User Interface DesignDocument30 pagesElements of User Interface DesignRomer Garcia100% (1)
- Mission: Children'SDocument36 pagesMission: Children'SWillian A. Palacio MurilloPas encore d'évaluation
- Analysis of The Style and Terminology Problems in Translating Legal TextsDocument19 pagesAnalysis of The Style and Terminology Problems in Translating Legal TextsMarvin EugenioPas encore d'évaluation
- M-10 Content+Previous Years QuestionDocument65 pagesM-10 Content+Previous Years QuestionOnline Physics Care by Syed Al-NahiyanPas encore d'évaluation
- Discoid Lupus Erythematosus - Background, Etiology, EpidemiologyDocument8 pagesDiscoid Lupus Erythematosus - Background, Etiology, EpidemiologyJair MathewsPas encore d'évaluation
- Unit - 3 Consignment: Learning OutcomesDocument36 pagesUnit - 3 Consignment: Learning OutcomesPrathamesh KamblePas encore d'évaluation
- Acadcalendar 2010-2011Document2 pagesAcadcalendar 2010-2011chantel_o12100% (1)
- 5 - Data Room Procedure TemplatesDocument8 pages5 - Data Room Procedure TemplatesnajahPas encore d'évaluation
- Compiler Design MCQ Question Bank Last Update 29-Dec-20202 Page 1 of 18Document18 pagesCompiler Design MCQ Question Bank Last Update 29-Dec-20202 Page 1 of 18SOMENATH ROY CHOUDHURYPas encore d'évaluation
- Progress Test 1 Units 1-6: Exercise 1 Personal InformationDocument3 pagesProgress Test 1 Units 1-6: Exercise 1 Personal InformationLuis Villaverde VerasteguiPas encore d'évaluation