Vous aimerez peut-être aussi
- HGVSJDocument2 pagesHGVSJRhod Bernaldez EstaPas encore d'évaluation
- Statistics PDFDocument54 pagesStatistics PDFRhod Bernaldez EstaPas encore d'évaluation
- Patient Safety Culture in Primary Care: Natasha VerbakelDocument176 pagesPatient Safety Culture in Primary Care: Natasha VerbakelRhod Bernaldez EstaPas encore d'évaluation
- NursingDocument1 pageNursingRhod Bernaldez EstaPas encore d'évaluation
- Carrebean SeaDocument7 pagesCarrebean SeaRhod Bernaldez Esta100% (1)
- Perceive/observe It. Please Answer All Items On This Sheet. If An Item Is Irrelevant, or IfDocument3 pagesPerceive/observe It. Please Answer All Items On This Sheet. If An Item Is Irrelevant, or IfRhod Bernaldez EstaPas encore d'évaluation
- Grenada History, Geography, Politics and EconomyDocument2 pagesGrenada History, Geography, Politics and EconomyRhod Bernaldez EstaPas encore d'évaluation
- Official Receipt PDFDocument1 pageOfficial Receipt PDFRhod Bernaldez EstaPas encore d'évaluation
- 2nd Patient Safety Congress RegistrationDocument1 page2nd Patient Safety Congress RegistrationRhod Bernaldez EstaPas encore d'évaluation
- Erastus Perceptions 2018 PDFDocument105 pagesErastus Perceptions 2018 PDFRhod Bernaldez EstaPas encore d'évaluation
- RHOD Seniority Complex Semi FinalDocument39 pagesRHOD Seniority Complex Semi FinalRhod Bernaldez EstaPas encore d'évaluation
- Radically Redesigning: Patient SafetyDocument9 pagesRadically Redesigning: Patient SafetyRhod Bernaldez EstaPas encore d'évaluation
- Sops Hospital Survey: Language: EnglishDocument6 pagesSops Hospital Survey: Language: EnglishNoviyanti LindaPas encore d'évaluation
- Leadership DevelopmentDocument2 pagesLeadership DevelopmentRhod Bernaldez EstaPas encore d'évaluation
- AHRQ Patient Safety Culture Improvement PlanDocument4 pagesAHRQ Patient Safety Culture Improvement PlanRhod Bernaldez EstaPas encore d'évaluation
- Patient Safety in Primary Healthcare A Review of The Literature August 2015Document160 pagesPatient Safety in Primary Healthcare A Review of The Literature August 2015Rhod Bernaldez EstaPas encore d'évaluation
- Facil Scan FormDocument7 pagesFacil Scan FormJoe ThesecondmonthPas encore d'évaluation
- Patient Safety Incident Reporting - Canadian Health SystemDocument13 pagesPatient Safety Incident Reporting - Canadian Health SystemRhod Bernaldez EstaPas encore d'évaluation
- Relationship Between Patient Safety Culture and Safety Outcome Measures Among NursesDocument80 pagesRelationship Between Patient Safety Culture and Safety Outcome Measures Among NursesRhod Bernaldez EstaPas encore d'évaluation
- MHD Mission VisionDocument1 pageMHD Mission VisionRhod Bernaldez EstaPas encore d'évaluation
- Fallpxtool 1 BDocument2 pagesFallpxtool 1 BRhod Bernaldez EstaPas encore d'évaluation
- Gardner-Webb University Digital Commons at Gardner-Webb UniversityDocument132 pagesGardner-Webb University Digital Commons at Gardner-Webb UniversityRhod Bernaldez EstaPas encore d'évaluation
- Control of Documented Information Procedure SampleDocument4 pagesControl of Documented Information Procedure Sampleingventor0% (1)
- Nurses' Perceptions of Patient Safety Culture in Oman: Fatma Al Dhabbari MSC, Pgd. BSC (Hons), R.G.NDocument3 pagesNurses' Perceptions of Patient Safety Culture in Oman: Fatma Al Dhabbari MSC, Pgd. BSC (Hons), R.G.NRhod Bernaldez EstaPas encore d'évaluation
- Objectives 2. Scope 3. Responsibilities 4. Records and References 5. Procedure Details Page No. Rev. No. Effectivity Nature of ChangeDocument8 pagesObjectives 2. Scope 3. Responsibilities 4. Records and References 5. Procedure Details Page No. Rev. No. Effectivity Nature of ChangeRhod Bernaldez EstaPas encore d'évaluation
- NursingDocument1 pageNursingRhod Bernaldez EstaPas encore d'évaluation
- Perceived Safety Culture of Healthcare Providers in Hospitals in The PhilippinesDocument14 pagesPerceived Safety Culture of Healthcare Providers in Hospitals in The PhilippinesRhod Bernaldez EstaPas encore d'évaluation
- Icrd Vawc-1Document1 pageIcrd Vawc-1Rhod Bernaldez EstaPas encore d'évaluation
- Implementing Rules and Regulations of The Lending Company Regulation Act of 2007 Ra9474Document19 pagesImplementing Rules and Regulations of The Lending Company Regulation Act of 2007 Ra9474Lance DionelaPas encore d'évaluation
- Leadership DevelopmentDocument2 pagesLeadership DevelopmentRhod Bernaldez EstaPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Medicine List by AmirDocument39 pagesMedicine List by AmirNomAn JuTtPas encore d'évaluation
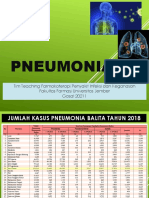
- Pneumonia: Tim Teaching Farmakoterapi Penyakit Infeksi Dan Keganasan Fakultas Farmasi Universitas Jember Gasal 20211Document67 pagesPneumonia: Tim Teaching Farmakoterapi Penyakit Infeksi Dan Keganasan Fakultas Farmasi Universitas Jember Gasal 20211Evie WulansariPas encore d'évaluation
- CPG Rational Antibiotic Utilisation in Selected Paediatric ConditionsDocument37 pagesCPG Rational Antibiotic Utilisation in Selected Paediatric ConditionsziggyshahdustPas encore d'évaluation
- Anti-Microbial USMLE Review: Active RecallDocument32 pagesAnti-Microbial USMLE Review: Active Recallmehrzi kamelPas encore d'évaluation
- Brain AbscessDocument13 pagesBrain Abscesskashim123Pas encore d'évaluation
- Cephalosporins GenerationDocument7 pagesCephalosporins GenerationSam SmileyPas encore d'évaluation
- Pharmacology Notes: EliminationDocument14 pagesPharmacology Notes: EliminationHaifa ibrahimPas encore d'évaluation
- Are Third Generation Cephalosporins Associated With A Bette - 2018 - Clinical MiDocument6 pagesAre Third Generation Cephalosporins Associated With A Bette - 2018 - Clinical MiRadia LachehebPas encore d'évaluation
- Acute Osteomyelitis: Diagnosis and ManagementDocument40 pagesAcute Osteomyelitis: Diagnosis and ManagementAnkit KarkiPas encore d'évaluation
- Antimicrobial Sensitivity of Most Commonly Isolated Bacteria From Feline Upper Respiratory Infection (URI)Document3 pagesAntimicrobial Sensitivity of Most Commonly Isolated Bacteria From Feline Upper Respiratory Infection (URI)KAREN LEE MEI FONGPas encore d'évaluation
- Community-Acquired Bacterial Meningitis in Adults: Review ArticleDocument10 pagesCommunity-Acquired Bacterial Meningitis in Adults: Review ArticleÁlvaro NBPas encore d'évaluation
- Rational Prescribing of Antibiotics in Infections in ChildrenDocument43 pagesRational Prescribing of Antibiotics in Infections in ChildrenVictor UmbuPas encore d'évaluation
- Cefotaxime 1g Powder For Solution For Injection or Infusion PL 14894 0397 Cefotaxime 2g Powder For Solution For Injection or Infusion PL 14894 0398Document48 pagesCefotaxime 1g Powder For Solution For Injection or Infusion PL 14894 0397 Cefotaxime 2g Powder For Solution For Injection or Infusion PL 14894 0398CongluanPas encore d'évaluation
- Beta Lactam AntibioticsDocument52 pagesBeta Lactam AntibioticsKaymie ReenPas encore d'évaluation
- Medication Guidelines Vol 1 Antimicrobial Prescribing v1.1 1Document77 pagesMedication Guidelines Vol 1 Antimicrobial Prescribing v1.1 1doodrillPas encore d'évaluation
- Hospital Antibiotic Policy: ST Helens and Knowsley Hospitals TrustDocument72 pagesHospital Antibiotic Policy: ST Helens and Knowsley Hospitals TrustDimas RfPas encore d'évaluation
- CeftriaxoneDocument7 pagesCeftriaxoneGreats HalomoanPas encore d'évaluation
- Pediatric Bacterial Meningitis in PhilippinesDocument27 pagesPediatric Bacterial Meningitis in Philippinesdranita@yahoo.comPas encore d'évaluation
- Indian JOurnal of PediatricsDocument8 pagesIndian JOurnal of Pediatricsliska ramdanawatiPas encore d'évaluation
- Pedia Care Study - Appendix B - Drug StudyDocument8 pagesPedia Care Study - Appendix B - Drug Studyryan100% (1)
- FormularyDocument123 pagesFormularyMuhammad Shakeel100% (3)
- Antibiotics: How Much Do You Know? Try Our Quiz For PrescribersDocument6 pagesAntibiotics: How Much Do You Know? Try Our Quiz For PrescribersSupratim SahaPas encore d'évaluation
- Pharmacy Training Book Topic GuideDocument355 pagesPharmacy Training Book Topic GuideHaneen HaneenPas encore d'évaluation
- Inhibitors of Bacterial Cell Wall Synthesis: Dr. Ndayisaba CorneilleDocument83 pagesInhibitors of Bacterial Cell Wall Synthesis: Dr. Ndayisaba CorneilleNdayisaba CorneillePas encore d'évaluation
- Christian Medical College Antimicrobial Therapy GuidelinesDocument43 pagesChristian Medical College Antimicrobial Therapy Guidelinesharshita guglaniPas encore d'évaluation
- Meningitis Pathophysiology PDFDocument59 pagesMeningitis Pathophysiology PDFpaswordnyalupa100% (1)
- Meningismus Vs MeningitisDocument19 pagesMeningismus Vs MeningitisRanna HertenizaPas encore d'évaluation
- Pediatric Drugs MKDDocument3 pagesPediatric Drugs MKDquixoticdreamer100% (7)
- Antibiotic Cross-Sensitivity Chart PDFDocument1 pageAntibiotic Cross-Sensitivity Chart PDFanareadsPas encore d'évaluation