Vous aimerez peut-être aussi
- MidtermDocument9 pagesMidtermjhouvanPas encore d'évaluation
- ch6 IM 1EDocument20 pagesch6 IM 1EJoan MaryPas encore d'évaluation
- CP Accounting MIdterm Review 15-16Document11 pagesCP Accounting MIdterm Review 15-16jhouvanPas encore d'évaluation
- FIN 311 SolutionDocument12 pagesFIN 311 SolutionMichael JohnsonPas encore d'évaluation
- Accounting 1Document17 pagesAccounting 1jhouvanPas encore d'évaluation
- Shapiro CapBgt IMDocument76 pagesShapiro CapBgt IMjhouvanPas encore d'évaluation
- Intermediate Accounting 2 2006 2007Document5 pagesIntermediate Accounting 2 2006 2007jhouvanPas encore d'évaluation
- 2009-05-01 063811 Multiple Choice-2Document12 pages2009-05-01 063811 Multiple Choice-2Andrea RobinsonPas encore d'évaluation
- UE-072300 Exh. No. - (CWK-1T) Testimony of Charles W. KingDocument36 pagesUE-072300 Exh. No. - (CWK-1T) Testimony of Charles W. KingjhouvanPas encore d'évaluation
- Kas 7 Accounting For Government Grants and Disclosure of Government AssistanceDocument15 pagesKas 7 Accounting For Government Grants and Disclosure of Government AssistancejhouvanPas encore d'évaluation
- Nasa Procedural Requirements: Responsible Office: Office of The Chief Financial OfficerDocument58 pagesNasa Procedural Requirements: Responsible Office: Office of The Chief Financial OfficerjhouvanPas encore d'évaluation
- FBLA Accounting Test PrepDocument10 pagesFBLA Accounting Test PrepjhouvanPas encore d'évaluation
- Appdx A - Final 08.01.11Document42 pagesAppdx A - Final 08.01.11jhouvanPas encore d'évaluation
- Act 6653 TgaaDocument11 pagesAct 6653 TgaajhouvanPas encore d'évaluation
- Fleet Acquistion and Disposal PolicyDocument3 pagesFleet Acquistion and Disposal PolicyjhouvanPas encore d'évaluation
- Capital Asset Management ProceduresDocument43 pagesCapital Asset Management Proceduresprsiva2420034066Pas encore d'évaluation
- MQ3 Spr08gDocument10 pagesMQ3 Spr08gjhouvanPas encore d'évaluation
- RG 08Document7 pagesRG 08jhouvanPas encore d'évaluation
- Accounting - Questions 010812Document4 pagesAccounting - Questions 010812jhouvanPas encore d'évaluation
- P2A Process - 2-Asset Control ProcessesDocument4 pagesP2A Process - 2-Asset Control ProcessesjhouvanPas encore d'évaluation
- Department of Finance Depreciation Instructions For Central Service AgenciesDocument1 pageDepartment of Finance Depreciation Instructions For Central Service AgenciesjhouvanPas encore d'évaluation
- Disposal of Gppe Scenario Board 5-3-12 CCDocument32 pagesDisposal of Gppe Scenario Board 5-3-12 CCjhouvanPas encore d'évaluation
- 7455 Accounting System For Fixed AssetsDocument3 pages7455 Accounting System For Fixed AssetsjhouvanPas encore d'évaluation
- 6e Ch09 PostDocument37 pages6e Ch09 PostjhouvanPas encore d'évaluation
- AIX Finance Lecture Student NotesDocument21 pagesAIX Finance Lecture Student NotesAsad MahmoodPas encore d'évaluation
- Assignment 3Document8 pagesAssignment 3jhouvanPas encore d'évaluation
- Review Accounting 1Document9 pagesReview Accounting 1jhouvanPas encore d'évaluation
- Depreciation MarkingDocument11 pagesDepreciation MarkingjhouvanPas encore d'évaluation
- Colorado Agriscience CurriculumDocument5 pagesColorado Agriscience CurriculumjhouvanPas encore d'évaluation
- Dfi 305 - DL Assg July 2012Document6 pagesDfi 305 - DL Assg July 2012jhouvanPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Difference: Inclusion and MainstreamingDocument2 pagesThe Difference: Inclusion and MainstreamingJay SproutPas encore d'évaluation
- 8 - CAMBRIDGE Hermeneutical InjusticeDocument21 pages8 - CAMBRIDGE Hermeneutical Injusticeleticia b.lPas encore d'évaluation
- Employing Persons With DisabilityDocument31 pagesEmploying Persons With Disabilitysam_dudePas encore d'évaluation
- Institutional Support for Disabled Human ResourcesDocument45 pagesInstitutional Support for Disabled Human ResourcesRokendro NongmaithemPas encore d'évaluation
- Special Education and Its CategoriesDocument7 pagesSpecial Education and Its Categoriesyfcb lamboPas encore d'évaluation
- NSF2006 PDFDocument401 pagesNSF2006 PDFbuiciagPas encore d'évaluation
- GradCatalog2011 2012Document219 pagesGradCatalog2011 2012Johnmael VazquezPas encore d'évaluation
- Retirement Plan Case StudyDocument30 pagesRetirement Plan Case Studyjeemee0320Pas encore d'évaluation
- Politics and Prosthetics - 150 Years of Disability in JapanDocument279 pagesPolitics and Prosthetics - 150 Years of Disability in JapanSaku DerePas encore d'évaluation
- Domestic Violence Aide-Memoire - Legal Guidance - The Crown Prosecution ServiceDocument20 pagesDomestic Violence Aide-Memoire - Legal Guidance - The Crown Prosecution Servicephoebe_62002239Pas encore d'évaluation
- 30320Document392 pages303209dsPas encore d'évaluation
- Ottawa County Agency GuideDocument102 pagesOttawa County Agency Guideapi-302699597Pas encore d'évaluation
- Levels of PreventionDocument75 pagesLevels of PreventionjayalakshmiPas encore d'évaluation
- Florence Gough, Amanda Brent, Susan Robinson One in Eleven Teaching Adolescents With A Language Learning Disability 2002Document156 pagesFlorence Gough, Amanda Brent, Susan Robinson One in Eleven Teaching Adolescents With A Language Learning Disability 2002Marijo100% (1)
- BMJ 334 7593 CR 00579Document10 pagesBMJ 334 7593 CR 00579RonaMaulidiaBakhitaPas encore d'évaluation
- Admission Evidence Exceptions Philippine Labor LawDocument43 pagesAdmission Evidence Exceptions Philippine Labor Lawying0240Pas encore d'évaluation
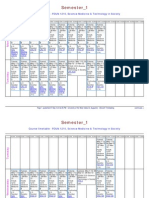
- Semester - 1: Course Timetable - FOUN 1210, Science Medicine & Technology in SocietyDocument5 pagesSemester - 1: Course Timetable - FOUN 1210, Science Medicine & Technology in SocietyAlexis SinghPas encore d'évaluation
- Accessibility Assignment 1 1Document7 pagesAccessibility Assignment 1 1api-301140443Pas encore d'évaluation
- OGUNSOLA and OLAOYE (2023) - Information Sharing Behaviour of Visually Impaired StudentsDocument25 pagesOGUNSOLA and OLAOYE (2023) - Information Sharing Behaviour of Visually Impaired StudentsKKPas encore d'évaluation
- Ucsp Q2 Module-1-7Document28 pagesUcsp Q2 Module-1-7Rose DiPas encore d'évaluation
- Handbook Inclusive EducationDocument194 pagesHandbook Inclusive EducationRUCHI MEHRA IPS Academy Indore100% (1)
- Achieving Inclusion For WebDocument16 pagesAchieving Inclusion For WebSteph GotlibPas encore d'évaluation
- Purposive Communication NotesDocument53 pagesPurposive Communication NotesJohara Bayabao85% (13)
- Labor Digest IDocument6 pagesLabor Digest IshezeharadeyahoocomPas encore d'évaluation
- School Health Services (3126135)Document129 pagesSchool Health Services (3126135)Prabhjeet100% (2)
- ADEC - Rawafed Private School 2015 2016Document20 pagesADEC - Rawafed Private School 2015 2016Edarabia.comPas encore d'évaluation
- Instructions For The: Modified Oswestry Low Back Pain Disability Index (Odi)Document3 pagesInstructions For The: Modified Oswestry Low Back Pain Disability Index (Odi)arjunjadeja08Pas encore d'évaluation
- Professional Development Plan For Co-TeachingDocument105 pagesProfessional Development Plan For Co-TeachingLina LilyPas encore d'évaluation
- The Grinch's Psychological ProfileDocument3 pagesThe Grinch's Psychological ProfileFrankiLevenson-Campanale100% (1)
- Emergency EvacuationDocument27 pagesEmergency EvacuationArif Staqvi Alfarizi100% (4)