Vous aimerez peut-être aussi
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
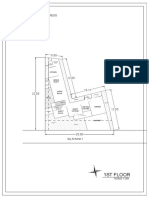
- 1St Floor: House On Paus Schematic Plan ProgressDocument2 pages1St Floor: House On Paus Schematic Plan Progressfiora.ladesvitaPas encore d'évaluation
- Gibson 2010Document19 pagesGibson 2010fiora.ladesvitaPas encore d'évaluation
- Determinants of Delay in Care Seeking Among Children Under Five With Fever in Dodoma Region, Central Tanzania: A Cross-Sectional StudyDocument10 pagesDeterminants of Delay in Care Seeking Among Children Under Five With Fever in Dodoma Region, Central Tanzania: A Cross-Sectional Studyfiora.ladesvitaPas encore d'évaluation
- Sex Differences in Cancer Risk and Survival: A Swedish Cohort StudyDocument11 pagesSex Differences in Cancer Risk and Survival: A Swedish Cohort Studyfiora.ladesvitaPas encore d'évaluation
- Childhood Illness Prevalence and Health Seeking Behavior Patterns in Rural TanzaniaDocument12 pagesChildhood Illness Prevalence and Health Seeking Behavior Patterns in Rural Tanzaniafiora.ladesvitaPas encore d'évaluation
- 2015 Conference 10Document11 pages2015 Conference 10fiora.ladesvitaPas encore d'évaluation
- Medicalscience: EcancerDocument7 pagesMedicalscience: Ecancerfiora.ladesvitaPas encore d'évaluation
- Caring: Prof. Dr. Budi Anna Keliat, MappscDocument59 pagesCaring: Prof. Dr. Budi Anna Keliat, Mappscfiora.ladesvitaPas encore d'évaluation
- Ambulatory Care Nursing: Coming Soon!Document16 pagesAmbulatory Care Nursing: Coming Soon!fiora.ladesvitaPas encore d'évaluation
- Assessment Rating ScaleDocument8 pagesAssessment Rating Scalefiora.ladesvitaPas encore d'évaluation
- Anderson2004 PDFDocument7 pagesAnderson2004 PDFfiora.ladesvitaPas encore d'évaluation
- Sistematic Review HoneyDocument159 pagesSistematic Review Honeyfiora.ladesvitaPas encore d'évaluation
- Living With Kidney DiseaseDocument96 pagesLiving With Kidney Diseasefiora.ladesvitaPas encore d'évaluation
- Idiom Meaning Examples: Toefl PreparationDocument4 pagesIdiom Meaning Examples: Toefl Preparationfiora.ladesvitaPas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Manuale捲板機Document96 pagesManuale捲板機Andy WuPas encore d'évaluation
- SAP Logistics Process ScopeDocument3 pagesSAP Logistics Process ScopecasiloPas encore d'évaluation
- Regional Trial Court National Capital Judicial Region: ComplainantDocument5 pagesRegional Trial Court National Capital Judicial Region: ComplainantNeil Patrick QuiniquiniPas encore d'évaluation
- Sample Paper For Professional Ethics in Accounting and FinanceDocument6 pagesSample Paper For Professional Ethics in Accounting and FinanceWinnieOngPas encore d'évaluation
- Engineering Discourse Communities RMDocument4 pagesEngineering Discourse Communities RMapi-336463296Pas encore d'évaluation
- 2020 LBG q1 Ims Pillar 3 DisclosuresDocument8 pages2020 LBG q1 Ims Pillar 3 DisclosuressaxobobPas encore d'évaluation
- Natural Gas DistributionDocument46 pagesNatural Gas DistributionscribdmisraPas encore d'évaluation
- Lescture OPACDocument5 pagesLescture OPACAgulto, Ivan R.Pas encore d'évaluation
- 2016 Lesson 9Document34 pages2016 Lesson 9Junas Jr LaputPas encore d'évaluation
- Deferred Tax QsDocument4 pagesDeferred Tax QsDaood AbdullahPas encore d'évaluation
- L-M349 (L1b1a) Kenézy Ancestral JourneyDocument20 pagesL-M349 (L1b1a) Kenézy Ancestral JourneyGábor Balogh100% (2)
- Price and Output Determination Under OligopolyDocument26 pagesPrice and Output Determination Under OligopolySangitha Nadar100% (1)
- B2 UNIT 4 Test StandardDocument6 pagesB2 UNIT 4 Test StandardВладимир РанцовPas encore d'évaluation
- Ealpha - Week 4 - Half A Day - ForeshadowingDocument2 pagesEalpha - Week 4 - Half A Day - ForeshadowingaalshehabPas encore d'évaluation
- Enzyme Kinetics Principles and MethodsDocument268 pagesEnzyme Kinetics Principles and MethodsCarlos Carinelli100% (4)
- HCT Baniqued P.D.E. Paper1 Version3 FullpaperDocument8 pagesHCT Baniqued P.D.E. Paper1 Version3 FullpaperJoshua HernandezPas encore d'évaluation
- Internship Proposal FormDocument3 pagesInternship Proposal FormMuhammad FidaPas encore d'évaluation
- Zimbabwe National Code Ccorporate GovernanceDocument96 pagesZimbabwe National Code Ccorporate GovernanceHerbert NgwaraiPas encore d'évaluation
- MAPEH Q4 ScriptDocument4 pagesMAPEH Q4 Scriptcharice maanoPas encore d'évaluation
- Uplifting Hauora Maori RealDocument32 pagesUplifting Hauora Maori RealFano AsiataPas encore d'évaluation
- Arizona History and Social Science StandardsDocument57 pagesArizona History and Social Science StandardsKJZZ PhoenixPas encore d'évaluation
- Settlement Geography: Unit No-1&2Document11 pagesSettlement Geography: Unit No-1&2Arindam RoulPas encore d'évaluation
- 10 Biological-HazardsDocument31 pages10 Biological-HazardsjvPas encore d'évaluation
- Soal Materi 1 KLS X IntroductionDocument2 pagesSoal Materi 1 KLS X IntroductionFira AnandaPas encore d'évaluation
- AutoPIPE Tutorial PDFDocument156 pagesAutoPIPE Tutorial PDFdhaktodesatyajitPas encore d'évaluation
- Moatiz Riaz - Area Sales ManagerDocument1 pageMoatiz Riaz - Area Sales ManagerMoatiz RiazPas encore d'évaluation
- Ra 9293 Amending Ra 7836Document2 pagesRa 9293 Amending Ra 7836vonoblessePas encore d'évaluation
- Hitachi Zx330 3 Series Hydraulic ExcavatorDocument15 pagesHitachi Zx330 3 Series Hydraulic ExcavatorAgung ArdhanaPas encore d'évaluation
- Architecture As Interface - Healing Architecture For Epatients. In: Healing Architecture. Hrsg. Nickl-Weller. 2013Document6 pagesArchitecture As Interface - Healing Architecture For Epatients. In: Healing Architecture. Hrsg. Nickl-Weller. 2013Asmaa AyadPas encore d'évaluation
- 10 Rules of Statcon by Atty Marcus NeelyDocument4 pages10 Rules of Statcon by Atty Marcus NeelyMorin OcoPas encore d'évaluation