Vous aimerez peut-être aussi
- Nucleus Gracilis and CuneatusDocument52 pagesNucleus Gracilis and CuneatusBeryl MarshallPas encore d'évaluation
- ENT 300 Individual Assessment-Personal Entrepreneurial CompetenciesDocument8 pagesENT 300 Individual Assessment-Personal Entrepreneurial CompetenciesAbu Ammar Al-hakimPas encore d'évaluation
- 2 To 20 Years - Girls Stature-For-Age and Weight-For-Age PercentilesDocument1 page2 To 20 Years - Girls Stature-For-Age and Weight-For-Age PercentilesRajalakshmi Vengadasamy0% (1)
- Sonographic Detection of Central Nervous System Defects in The First Trimester of PregnancyDocument8 pagesSonographic Detection of Central Nervous System Defects in The First Trimester of PregnancyVishnu priya kokkulaPas encore d'évaluation
- ISUOG - Fetal Nervous System ExaminationDocument8 pagesISUOG - Fetal Nervous System ExaminationAzucenaPas encore d'évaluation
- Tfus Part 1Document10 pagesTfus Part 1Seyfullah Halit KaragözPas encore d'évaluation
- 33 HR 1 AsdadDocument3 pages33 HR 1 AsdadbingchillingPas encore d'évaluation
- Featured Applied Radiology Article: Pediatric Neuroradiology Part 1 - Embryo Logic Basis For Brain MalformationDocument12 pagesFeatured Applied Radiology Article: Pediatric Neuroradiology Part 1 - Embryo Logic Basis For Brain MalformationradRounds Radiology NetworkPas encore d'évaluation
- DEVELOPMENT NERVOUS SYSTEM Brain Face PDFDocument15 pagesDEVELOPMENT NERVOUS SYSTEM Brain Face PDFChidera EmmanuelPas encore d'évaluation
- 2 Head and Neck Anatomy SPTH 204Document79 pages2 Head and Neck Anatomy SPTH 204Noor KhalilPas encore d'évaluation
- Cerebelo: Dr. J.J. Colon R6 C.M.N. La RazaDocument74 pagesCerebelo: Dr. J.J. Colon R6 C.M.N. La RazaJose Jesus ColonPas encore d'évaluation
- CNS DevelopmentDocument158 pagesCNS DevelopmentMubashir SiyalPas encore d'évaluation
- Embryology-Development of Central Nervous SystemDocument28 pagesEmbryology-Development of Central Nervous Systemtenshi315Pas encore d'évaluation
- Development of The NSDocument7 pagesDevelopment of The NSJean Pierre Chastre LuzaPas encore d'évaluation
- Review Article: Mohammad SarwarDocument17 pagesReview Article: Mohammad SarwarRuslan MilevskyPas encore d'évaluation
- Nervous SystemDocument296 pagesNervous SystemDr. Serin KuriakosePas encore d'évaluation
- Neuroanatomy of The Zebrafish Brain - A Topological Atlas 1996Document141 pagesNeuroanatomy of The Zebrafish Brain - A Topological Atlas 1996Daniel RuizPas encore d'évaluation
- Neuroanatomy, Cerebellar Dysfunction: Gross AnatomyDocument5 pagesNeuroanatomy, Cerebellar Dysfunction: Gross AnatomyANISA RIFKA RIDHOPas encore d'évaluation
- The CerebellumDocument5 pagesThe CerebellumAndrew BarryPas encore d'évaluation
- Development of The Central Nervous System: Consists of The Brain and Spinal Cord Derived From The Neural TubeDocument42 pagesDevelopment of The Central Nervous System: Consists of The Brain and Spinal Cord Derived From The Neural TubeZyra PerolPas encore d'évaluation
- Contribution of Transvaginal High-Resolution Ultra PDFDocument8 pagesContribution of Transvaginal High-Resolution Ultra PDFManikandan PerumalPas encore d'évaluation
- Key Points:: Questions For StudentsDocument12 pagesKey Points:: Questions For Studentssimi yPas encore d'évaluation
- Purves - Neuroanatomy (Semana 4)Document43 pagesPurves - Neuroanatomy (Semana 4)valentina castilloPas encore d'évaluation
- Bahan Saraf 02Document13 pagesBahan Saraf 02Dipo SiahaanPas encore d'évaluation
- 33 HRDocument4 pages33 HRleyPas encore d'évaluation
- Ebook Psychology Psyc2020 Psyc2021 Custom Edition by Schutte E Ed Et A PDF Full Chapter PDFDocument67 pagesEbook Psychology Psyc2020 Psyc2021 Custom Edition by Schutte E Ed Et A PDF Full Chapter PDFedward.bittner820100% (26)
- Arteries and Veins of The Cerebellum: Original PaperDocument33 pagesArteries and Veins of The Cerebellum: Original PaperCan EkerPas encore d'évaluation
- Patterning The Developing DiencephalonDocument10 pagesPatterning The Developing DiencephalonAndres MoraPas encore d'évaluation
- Krigestin Et Al 2006, Neural Stem Cell PrgenitorDocument8 pagesKrigestin Et Al 2006, Neural Stem Cell PrgenitorSalma Moustafa MahmoudPas encore d'évaluation
- MeningesDocument2 pagesMeningesDurga MadhuriPas encore d'évaluation
- Ultrasonographic Evaluation of The Fetal Neural Axis: JournalsDocument10 pagesUltrasonographic Evaluation of The Fetal Neural Axis: Journalsdgina8800Pas encore d'évaluation
- Fetomaternal III (CNS and Fetal Brain Anomaly)Document67 pagesFetomaternal III (CNS and Fetal Brain Anomaly)Eka Handayani OktharinaPas encore d'évaluation
- 02 - CNS DevelopmentDocument3 pages02 - CNS DevelopmentCemre KuzeyPas encore d'évaluation
- EmbryologyDocument92 pagesEmbryologyLoveena SteadmanPas encore d'évaluation
- 48 Hrs 1 AsdDocument4 pages48 Hrs 1 AsdbingchillingPas encore d'évaluation
- OSCE Cerebellar Examination PDFDocument6 pagesOSCE Cerebellar Examination PDFriczen vilaPas encore d'évaluation
- Embryology Summary of Development Part 1 - 2019 - CNS, Axial SK, SK Muscle, SkinDocument9 pagesEmbryology Summary of Development Part 1 - 2019 - CNS, Axial SK, SK Muscle, Skindr.mumtaz09Pas encore d'évaluation
- Thespinalcord: A Review of Functional NeuroanatomyDocument18 pagesThespinalcord: A Review of Functional NeuroanatomyasfwegerePas encore d'évaluation
- Altmann 2001Document36 pagesAltmann 2001zsmm1993Pas encore d'évaluation
- 9w HoloprosencephalyDocument4 pages9w HoloprosencephalyVũ Quang ĐăngPas encore d'évaluation
- Frog EmbryosDocument43 pagesFrog EmbryosNics Martinez100% (7)
- Anatomy and Approaches Along The Cerebellar-Brainstem FissuresDocument16 pagesAnatomy and Approaches Along The Cerebellar-Brainstem Fissureskaan_yagmur7711Pas encore d'évaluation
- 2019 NEUR3005 3905 Hypothalamus - AggressionDocument34 pages2019 NEUR3005 3905 Hypothalamus - AggressionjacksonzchenPas encore d'évaluation
- Fig. 17.3B: RhombencephalonDocument2 pagesFig. 17.3B: RhombencephalonJSPas encore d'évaluation
- Department of Anatomy College of Medicine University of Ibadan Neuroanatomy Dissection of The BrainDocument22 pagesDepartment of Anatomy College of Medicine University of Ibadan Neuroanatomy Dissection of The BrainAbdulateef AdebisiPas encore d'évaluation
- Posterior Fontanelle Cranial Ultrasound: Anatotic and Sonographic CorrelationDocument12 pagesPosterior Fontanelle Cranial Ultrasound: Anatotic and Sonographic CorrelationDaniela CioboataPas encore d'évaluation
- Chick Embryo 72 HoursDocument48 pagesChick Embryo 72 HoursogheeluvPas encore d'évaluation
- Neonatal Cranial Sonography: A Concise Review For CliniciansDocument7 pagesNeonatal Cranial Sonography: A Concise Review For CliniciansDaniela CioboataPas encore d'évaluation
- Hubs2103 - Neural and Visceral AnatomyDocument153 pagesHubs2103 - Neural and Visceral AnatomyLuke ThomsonPas encore d'évaluation
- Article EmbriologyDocument6 pagesArticle Embriologycestrada10Pas encore d'évaluation
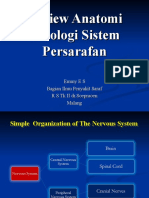
- Review Anatomi Fisiologi Sistem PersarafanDocument78 pagesReview Anatomi Fisiologi Sistem PersarafanNisa FathonahPas encore d'évaluation
- Ventricles: M N C CDocument3 pagesVentricles: M N C CEijunPas encore d'évaluation
- Lymphatic FilariasisDocument17 pagesLymphatic FilariasisSelvaPas encore d'évaluation
- Leavitt 2005Document16 pagesLeavitt 2005qr7bht566gPas encore d'évaluation
- Embriologi Brain and SpineDocument18 pagesEmbriologi Brain and SpineJunus EufrataPas encore d'évaluation
- Lesson 3.Document15 pagesLesson 3.Maedel Rose EsguerraPas encore d'évaluation
- BRAINSTEMDocument17 pagesBRAINSTEMaroosadilbar27Pas encore d'évaluation
- Overview: Functions of The CerebellumDocument17 pagesOverview: Functions of The CerebellumMohd Fitri ShahruddinPas encore d'évaluation
- 5 Pelvic Floor AJ 2022 v2Document79 pages5 Pelvic Floor AJ 2022 v2Husam OsmanPas encore d'évaluation
- 8 Brainstem 2Document20 pages8 Brainstem 2sjs6r8wwv9Pas encore d'évaluation
- Laporan Nbss ...Document88 pagesLaporan Nbss ...Nita AndriyaniPas encore d'évaluation
- Top 100 Chemical CompaniesDocument11 pagesTop 100 Chemical Companiestawhide_islamicPas encore d'évaluation
- MSC-MEPC.2-Circ.17 - 2019 Guidelines For The Carriage of Blends OfBiofuels and Marpol Annex I Cargoes (Secretariat)Document4 pagesMSC-MEPC.2-Circ.17 - 2019 Guidelines For The Carriage of Blends OfBiofuels and Marpol Annex I Cargoes (Secretariat)DeepakPas encore d'évaluation
- I I I I: Peroxid.Q!Document2 pagesI I I I: Peroxid.Q!Diego PradelPas encore d'évaluation
- 385C Waw1-Up PDFDocument4 pages385C Waw1-Up PDFJUNA RUSANDI SPas encore d'évaluation
- Introduction To Retail LoansDocument2 pagesIntroduction To Retail LoansSameer ShahPas encore d'évaluation
- Cyclic MeditationDocument8 pagesCyclic MeditationSatadal GuptaPas encore d'évaluation
- Question Answers of Chapter 13 Class 5Document6 pagesQuestion Answers of Chapter 13 Class 5SuvashreePradhanPas encore d'évaluation
- Feasibility Study For Cowboy Cricket Farms Final Report: Prepared For Prospera Business Network Bozeman, MTDocument42 pagesFeasibility Study For Cowboy Cricket Farms Final Report: Prepared For Prospera Business Network Bozeman, MTMyself IrenePas encore d'évaluation
- Measuring Temperature - Platinum Resistance ThermometersDocument3 pagesMeasuring Temperature - Platinum Resistance Thermometersdark*nightPas encore d'évaluation
- Jan 25th 6 TicketsDocument2 pagesJan 25th 6 TicketsMohan Raj VeerasamiPas encore d'évaluation
- ALE Manual For LaserScope Arc Lamp Power SupplyDocument34 pagesALE Manual For LaserScope Arc Lamp Power SupplyKen DizzeruPas encore d'évaluation
- Instant Download Ebook PDF Ecology Concepts and Applications 8th Edition PDF ScribdDocument41 pagesInstant Download Ebook PDF Ecology Concepts and Applications 8th Edition PDF Scribdsteven.cross256100% (45)
- Marketing Channels: A Strategic Tool of Growing Importance For The Next MillenniumDocument59 pagesMarketing Channels: A Strategic Tool of Growing Importance For The Next MillenniumAnonymous ibmeej9Pas encore d'évaluation
- Epreuve Anglais EG@2022Document12 pagesEpreuve Anglais EG@2022Tresor SokoudjouPas encore d'évaluation
- WHO Guidelines For Drinking Water: Parameters Standard Limits As Per WHO Guidelines (MG/L)Document3 pagesWHO Guidelines For Drinking Water: Parameters Standard Limits As Per WHO Guidelines (MG/L)114912Pas encore d'évaluation
- Dreaded Attack - Voyages Community Map Rules v1Document2 pagesDreaded Attack - Voyages Community Map Rules v1jPas encore d'évaluation
- General Chemistry 2 Q1 Lesson 5 Endothermic and Exotheric Reaction and Heating and Cooling CurveDocument19 pagesGeneral Chemistry 2 Q1 Lesson 5 Endothermic and Exotheric Reaction and Heating and Cooling CurveJolo Allexice R. PinedaPas encore d'évaluation
- CN1111 Tutorial 4 QuestionDocument3 pagesCN1111 Tutorial 4 Questionthenewperson0% (1)
- Mozal Finance EXCEL Group 15dec2013Document15 pagesMozal Finance EXCEL Group 15dec2013Abhijit TailangPas encore d'évaluation
- HRMDocument118 pagesHRMKarthic KasiliaPas encore d'évaluation
- EKRP311 Vc-Jun2022Document3 pagesEKRP311 Vc-Jun2022dfmosesi78Pas encore d'évaluation
- Application of Geoelectric Method For GroundwaterDocument11 pagesApplication of Geoelectric Method For GroundwaterMunther DhahirPas encore d'évaluation
- BIAN How To Guide Developing Content V7.0 Final V1.0 PDFDocument72 pagesBIAN How To Guide Developing Content V7.0 Final V1.0 PDFميلاد نوروزي رهبرPas encore d'évaluation
- Bcci ScandalDocument6 pagesBcci ScandalNausaf AhmedPas encore d'évaluation
- Biological Assets Sample ProblemsDocument4 pagesBiological Assets Sample ProblemsKathleenPas encore d'évaluation
- Smart Protein Plant Based Food Sector Report 2Document199 pagesSmart Protein Plant Based Food Sector Report 2campeon00magnatesPas encore d'évaluation
- ADC of PIC MicrocontrollerDocument4 pagesADC of PIC Microcontrollerkillbill100% (2)
- Walking in Space - Lyrics and Chord PatternDocument2 pagesWalking in Space - Lyrics and Chord Patternjohn smithPas encore d'évaluation