Vous aimerez peut-être aussi
- Adult Infectious Disease Bulletpoints HandbookD'EverandAdult Infectious Disease Bulletpoints HandbookÉvaluation : 4.5 sur 5 étoiles4.5/5 (9)
- Ebola: The Natural and Human History of A Deadly Virus (Norton, October 2014), by David QuammenDocument4 pagesEbola: The Natural and Human History of A Deadly Virus (Norton, October 2014), by David QuammenThe World50% (4)
- Rife FrequenciesDocument228 pagesRife Frequenciessvdmfgbc100% (2)
- Pneumonia: Fever Cough Breathlessnes S DR J Pap/ich/ GMC Kottayam/19723Document4 pagesPneumonia: Fever Cough Breathlessnes S DR J Pap/ich/ GMC Kottayam/19723Firdouse ShajiPas encore d'évaluation
- NICU ABX ChartDocument11 pagesNICU ABX ChartdrchiPas encore d'évaluation
- Bone and Joint Infections BNHFT 2010 PDFDocument3 pagesBone and Joint Infections BNHFT 2010 PDFDanissa Fidia PuteriPas encore d'évaluation
- 5 Cefuroxime Drug StudyDocument4 pages5 Cefuroxime Drug Studyshadow gonzalezPas encore d'évaluation
- Antibiotic Guidelines For PediatricsDocument33 pagesAntibiotic Guidelines For PediatricsVarshini Tamil SelvanPas encore d'évaluation
- Amoxicillin (Amoxycillin) : PresentationDocument4 pagesAmoxicillin (Amoxycillin) : PresentationRavikiran SuryanarayanamurthyPas encore d'évaluation
- Any Up-Dates Are To Be Completed in Different Color Ink. The Student Is Expected To Document All Meds The Client Is Currently ReceivingDocument1 pageAny Up-Dates Are To Be Completed in Different Color Ink. The Student Is Expected To Document All Meds The Client Is Currently Receivinggeorgeloto12Pas encore d'évaluation
- Management of CAP in Adults - Ontario GovernmentDocument2 pagesManagement of CAP in Adults - Ontario GovernmentSukhvir AujlaPas encore d'évaluation
- Respiratory Tract Infections - Med DidacticsDocument59 pagesRespiratory Tract Infections - Med Didacticsapi-649060644Pas encore d'évaluation
- Guide of MedicationDocument4 pagesGuide of MedicationتَبٰارْكـPas encore d'évaluation
- Pediatric Guidelines: Head and Neck Infections - MastoiditisDocument3 pagesPediatric Guidelines: Head and Neck Infections - MastoiditisJr SparkPas encore d'évaluation
- AB Doses Common DiseasesDocument15 pagesAB Doses Common DiseasesTariqPas encore d'évaluation
- AntibioticsDocument17 pagesAntibioticsnehal.nehal92Pas encore d'évaluation
- Paediatric Antibiotic TeddyDocument1 pagePaediatric Antibiotic Teddyayu fitrianiPas encore d'évaluation
- Aminoglycosides: Under Supervision ofDocument5 pagesAminoglycosides: Under Supervision ofKhaled NagyPas encore d'évaluation
- Penicillins 1Document30 pagesPenicillins 1John PaulPas encore d'évaluation
- Notebook PDFDocument4 pagesNotebook PDFCJMALPas encore d'évaluation
- UAW Respiratory Antimicrobial Pharm Guide MedstuDocument19 pagesUAW Respiratory Antimicrobial Pharm Guide MedstuNabeel ShahzadPas encore d'évaluation
- Antibiotics Guide 2013Document30 pagesAntibiotics Guide 2013Stefani NoviliaPas encore d'évaluation
- IMG EmpAposterDocument1 pageIMG EmpAposterChiu LeoPas encore d'évaluation
- VancomycinDocument1 pageVancomycinJUSTINE ALLYSA MAY CASTILLOPas encore d'évaluation
- Urinary Tract InfectionsDocument15 pagesUrinary Tract InfectionsAnonymous elSqPhzKPas encore d'évaluation
- COVID19 Management Algorithm 22042021 v1Document1 pageCOVID19 Management Algorithm 22042021 v1shivani shindePas encore d'évaluation
- Parasitic WormsDocument4 pagesParasitic WormsEricPas encore d'évaluation
- CASE PRESENTATION PneumoniaDocument13 pagesCASE PRESENTATION PneumoniaHari Singh RathorePas encore d'évaluation
- Guidelines For Treatment of Intra-Abdominal Infections in AdultsDocument10 pagesGuidelines For Treatment of Intra-Abdominal Infections in AdultsPratama InsaniPas encore d'évaluation
- NAG Central Nervous System Infections As of Nov 2017Document9 pagesNAG Central Nervous System Infections As of Nov 2017Rhod Bernaldez EstaPas encore d'évaluation
- Cephalexin Drug Study RNpedia ComDocument2 pagesCephalexin Drug Study RNpedia ComKatyana Cesar100% (1)
- Case Study 4 Drug StudyDocument9 pagesCase Study 4 Drug StudyMontero, Ma. Cecilia - BSN 3-BPas encore d'évaluation
- Gentamicin Sulfate-Drug StudyDocument3 pagesGentamicin Sulfate-Drug StudyDaisy Palisoc82% (11)
- Antibiotic Policy - Final GovtMP - 211215 - 121049Document40 pagesAntibiotic Policy - Final GovtMP - 211215 - 121049Charchit MehtaPas encore d'évaluation
- Pediatric Hospital-Acquired and Ventilator-Associated Pneumonia Topic DiscussionDocument5 pagesPediatric Hospital-Acquired and Ventilator-Associated Pneumonia Topic Discussionapi-602288180Pas encore d'évaluation
- Empirical Antibiotic Therapy in Children v7 Exp 31 Dec 2020Document2 pagesEmpirical Antibiotic Therapy in Children v7 Exp 31 Dec 2020Mohamad MostafaPas encore d'évaluation
- GHC Lower Respiratory Tract Antimicrobial Guideline V 3 FinalDocument19 pagesGHC Lower Respiratory Tract Antimicrobial Guideline V 3 FinalNicthe Ruiz RodríguezPas encore d'évaluation
- HSB Pneumonia Antibiotic AlgorithmDocument4 pagesHSB Pneumonia Antibiotic AlgorithmDr.Senthil KumarPas encore d'évaluation
- Medication PicuDocument2 pagesMedication PicuSweety KurnPas encore d'évaluation
- Antibiotic Treatment Guidelines For Urinary Tract Infections in Children (60 Days Through 17 Years)Document3 pagesAntibiotic Treatment Guidelines For Urinary Tract Infections in Children (60 Days Through 17 Years)Zahid AbbasPas encore d'évaluation
- Severe Sepsis and Septic Shock Antibiotic Guide: Community AcquiredDocument6 pagesSevere Sepsis and Septic Shock Antibiotic Guide: Community AcquiredAnonymous G6zDTD2yPas encore d'évaluation
- Pneumonia ADULTDocument6 pagesPneumonia ADULTSebastian TjuwatjaPas encore d'évaluation
- Zinnat TabletsDocument5 pagesZinnat TabletsAndrei Marian BorcescuPas encore d'évaluation
- Antibiotka PicuDocument4 pagesAntibiotka Picusunu rachmat100% (1)
- Drug Study - AmoxicillinDocument2 pagesDrug Study - AmoxicillinVANESSA PAULA ALGADORPas encore d'évaluation
- Emma Best, Simon Briggs, Rosemary Ikram, Mark Thomas - Antibiotics - Choices For Common Infections 2013 Edition (BPAC NZ) (2013, BPAC NZ)Document28 pagesEmma Best, Simon Briggs, Rosemary Ikram, Mark Thomas - Antibiotics - Choices For Common Infections 2013 Edition (BPAC NZ) (2013, BPAC NZ)igd rsudcpPas encore d'évaluation
- 2RS. 3 PneumoniaDocument33 pages2RS. 3 PneumoniaMuath AlqarniPas encore d'évaluation
- Chapter 2 - Antimicrobial Therapy For Head and Neck InfectionDocument13 pagesChapter 2 - Antimicrobial Therapy For Head and Neck InfectionMario CastanedaPas encore d'évaluation
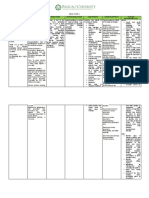
- Drug Name Mode of Action Indications/Contraindicati Ons Adverse Effects Nursing Considerations BeforeDocument2 pagesDrug Name Mode of Action Indications/Contraindicati Ons Adverse Effects Nursing Considerations BeforeMikko McDonie VeloriaPas encore d'évaluation
- Acute Upper Respiratory Tract Infection. 1Document20 pagesAcute Upper Respiratory Tract Infection. 1Joana Carolina QuiambaoPas encore d'évaluation
- Antibiotic Hospital ManDocument1 pageAntibiotic Hospital Manarshiya.manasekiPas encore d'évaluation
- Central Nervous System InfectionsDocument9 pagesCentral Nervous System InfectionsSaddamPas encore d'évaluation
- Infectious Gastroenteritis BaDocument1 pageInfectious Gastroenteritis BafionaPas encore d'évaluation
- Pneumonia Treatment Algorithm With Addendum For Aspiration 2015-2016.01.19Document2 pagesPneumonia Treatment Algorithm With Addendum For Aspiration 2015-2016.01.19Irsalina TriastutikPas encore d'évaluation
- Pharm: Antibacteria/Antiviral/AntifungalDocument19 pagesPharm: Antibacteria/Antiviral/AntifungalNathan BarrerasPas encore d'évaluation
- AMPXICILLINDocument3 pagesAMPXICILLINPark JeongyeonPas encore d'évaluation
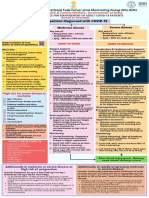
- Adult Patient Diagnosed With COVID-19: Ministry of Health & Family Welfare, Government of IndiaDocument1 pageAdult Patient Diagnosed With COVID-19: Ministry of Health & Family Welfare, Government of Indiapramodbankhele3845Pas encore d'évaluation
- CNS Infection GuidanceDocument2 pagesCNS Infection GuidanceGus LionsPas encore d'évaluation
- Empiric Antibiotic ListDocument2 pagesEmpiric Antibiotic ListpasswordPas encore d'évaluation
- Roundworm Infections, A Simple Guide To The Condition, Treatment And Related ConditionsD'EverandRoundworm Infections, A Simple Guide To The Condition, Treatment And Related ConditionsPas encore d'évaluation
- Ulcerative Colitis, A Simple Guide To The Condition, Treatment And Related ConditionsD'EverandUlcerative Colitis, A Simple Guide To The Condition, Treatment And Related ConditionsPas encore d'évaluation
- Agranulocytosis, A Simple Guide to The Condition, Diagnosis, Treatment And Related ConditionsD'EverandAgranulocytosis, A Simple Guide to The Condition, Diagnosis, Treatment And Related ConditionsPas encore d'évaluation
- Bab Ii HNPDocument10 pagesBab Ii HNPSiti Hidayatul FitriPas encore d'évaluation
- International Journal of Pediatric OtorhinolaryngologyDocument10 pagesInternational Journal of Pediatric OtorhinolaryngologySiti Hidayatul FitriPas encore d'évaluation
- Fakultas Kedokteran Universitas AndalasDocument3 pagesFakultas Kedokteran Universitas AndalasSiti Hidayatul FitriPas encore d'évaluation
- Pelatihan Kader: Lampiran Uji StatistikDocument2 pagesPelatihan Kader: Lampiran Uji StatistikSiti Hidayatul FitriPas encore d'évaluation
- EbolaaDocument6 pagesEbolaaSiti Hidayatul FitriPas encore d'évaluation
- Cong GengueDocument4 pagesCong GengueSiti Hidayatul FitriPas encore d'évaluation
- KP 1.4.2.6 Kuliah 3. Kontrol Sistem PencernaanDocument23 pagesKP 1.4.2.6 Kuliah 3. Kontrol Sistem PencernaanSiti Hidayatul FitriPas encore d'évaluation
- Nasal-Septal Fractures: Francis B. Quinn, M.D. Herve' J. Leboeuf, M.DDocument26 pagesNasal-Septal Fractures: Francis B. Quinn, M.D. Herve' J. Leboeuf, M.DSiti Hidayatul FitriPas encore d'évaluation
- Risk Assessment Questionnaire For WorkersDocument2 pagesRisk Assessment Questionnaire For WorkersRichard R M ThodéPas encore d'évaluation
- Pendekatan Desain Dan Aplikasi Ruang Praktek Dokter Gigi Di Masa PandemiDocument13 pagesPendekatan Desain Dan Aplikasi Ruang Praktek Dokter Gigi Di Masa PandemiKeyla Maharani AddlewishPas encore d'évaluation
- VVMDocument2 pagesVVMJorry PoulosePas encore d'évaluation
- Stock 01 Des 22Document70 pagesStock 01 Des 22kaprodiS1 stikesalfatahPas encore d'évaluation
- COVID-19 Vaccine Booster Doses and Third Doses - COVID-19Document6 pagesCOVID-19 Vaccine Booster Doses and Third Doses - COVID-19Reynan MaurícioPas encore d'évaluation
- Sargam SoodDocument1 pageSargam SoodMayank JunejaPas encore d'évaluation
- F Template - Minor Quarantine Letter For Covid Close Contact - 09.03.2021Document2 pagesF Template - Minor Quarantine Letter For Covid Close Contact - 09.03.2021WXMIPas encore d'évaluation
- HepatomaDocument5 pagesHepatomaJose Emmanuel FranciaPas encore d'évaluation
- Poultry Prescription PDFDocument19 pagesPoultry Prescription PDFAnonymous UdZFdhcnPas encore d'évaluation
- Medical AsepsisDocument23 pagesMedical AsepsisRashid HussainPas encore d'évaluation
- Micro ParasitologyDocument5 pagesMicro ParasitologyPlzstudylav SyedPas encore d'évaluation
- Reading and Writing Skills Module 39999Document2 pagesReading and Writing Skills Module 39999Ericka Rivera SantosPas encore d'évaluation
- ClinicalStagesofHIVBiolixir Published2011Document4 pagesClinicalStagesofHIVBiolixir Published2011Lyzia AushaPas encore d'évaluation
- Form ICRADocument3 pagesForm ICRAlinda widiantiPas encore d'évaluation
- Italy Responds To COVID-19Document102 pagesItaly Responds To COVID-19Zerohedge100% (1)
- A. Cotton Blue: False TrueDocument5 pagesA. Cotton Blue: False TrueDevinViscars100% (1)
- Feed Additives, Antibodies, Poultry Vaccines 2023.3Document6 pagesFeed Additives, Antibodies, Poultry Vaccines 2023.3Bruce YangPas encore d'évaluation
- Prevention and Control of MalariaDocument53 pagesPrevention and Control of Malariaapi-3823785100% (1)
- Propuesta A The Dakota Building: Idioma Extranjero: Inglés. 2015/2016Document4 pagesPropuesta A The Dakota Building: Idioma Extranjero: Inglés. 2015/2016Monika PerezPas encore d'évaluation
- Kepositifan Induksi Sputum NaCl 3 Dan Teknik BroncDocument7 pagesKepositifan Induksi Sputum NaCl 3 Dan Teknik Broncvovinda rujianaPas encore d'évaluation
- Frequently Asked Questions (FAQ) : Communicable Disease Assessment & ImmunizationsDocument6 pagesFrequently Asked Questions (FAQ) : Communicable Disease Assessment & ImmunizationsmaiPas encore d'évaluation
- Duke Criteria For IE II - UpToDateDocument2 pagesDuke Criteria For IE II - UpToDateKavindu TennakoonPas encore d'évaluation
- What Is Polio?Document3 pagesWhat Is Polio?Yanna BaptistaPas encore d'évaluation
- Hubungan Dukungan Keluarga Dengan Kepatuhan Minum Obat Pada Penderita TB Paru Di Puskesmaspadang Bulan MedanDocument7 pagesHubungan Dukungan Keluarga Dengan Kepatuhan Minum Obat Pada Penderita TB Paru Di Puskesmaspadang Bulan MedanSiti KomariahPas encore d'évaluation
- Unit 1-Lecture 2 Basic Laboratory Safety: Contemporary Clinical Immunology and SerologyDocument107 pagesUnit 1-Lecture 2 Basic Laboratory Safety: Contemporary Clinical Immunology and SerologyBecky GoodwinPas encore d'évaluation
- Flu Religious ExemptionDocument3 pagesFlu Religious ExemptionFRANCHESCA DEL MUNDOPas encore d'évaluation
- Ipcn Edukasi JurnalDocument16 pagesIpcn Edukasi JurnalJono ParmiPas encore d'évaluation
- VaccineDocument17 pagesVaccineSamanta Jay RodriguezPas encore d'évaluation