Vous aimerez peut-être aussi
- Ma 05020Document11 pagesMa 05020Ayo MakanjuolaPas encore d'évaluation
- Laparoscopic AdrenalectomyDocument12 pagesLaparoscopic AdrenalectomyTay SalinasPas encore d'évaluation
- Botea Et Al Vertical Bipartition of The Right Anterior Section by Extraglissonian ApproachDocument15 pagesBotea Et Al Vertical Bipartition of The Right Anterior Section by Extraglissonian ApproachflorinscribdPas encore d'évaluation
- Bjs 9618Document3 pagesBjs 9618Mohammed FaragPas encore d'évaluation
- Extension of surgical indications for liver metastasesDocument21 pagesExtension of surgical indications for liver metastasesAni Riani SunartoPas encore d'évaluation
- Systematic Review Go WakaDocument8 pagesSystematic Review Go WakaNoemi Di FucciaPas encore d'évaluation
- Radical Surgery For Cancer of The Pancreas: Kothaj PDocument3 pagesRadical Surgery For Cancer of The Pancreas: Kothaj Pyacine26Pas encore d'évaluation
- Ahn 2011Document4 pagesAhn 2011Residentes PediatríaPas encore d'évaluation
- SMJ 60 247Document6 pagesSMJ 60 247Chee Yung NgPas encore d'évaluation
- International Journal of Surgery: SciencedirectDocument7 pagesInternational Journal of Surgery: SciencedirectFerdian PriantoPas encore d'évaluation
- Ninomiya 等 - 2020 - Clip on Staple Method to Prevent Bile Leakage in ADocument4 pagesNinomiya 等 - 2020 - Clip on Staple Method to Prevent Bile Leakage in A蔡一鹏Pas encore d'évaluation
- Kurum Boor 2016Document4 pagesKurum Boor 2016Chema ToledoPas encore d'évaluation
- Hepatectomía Laparoscópica : Laparoscopic HepatectomyDocument9 pagesHepatectomía Laparoscópica : Laparoscopic HepatectomyRudy GuarnizPas encore d'évaluation
- 1 s2.0 S101595841730622X MainDocument7 pages1 s2.0 S101595841730622X Mainyerich septaPas encore d'évaluation
- A Case Report of Liver Infiltration From A Large - 2024 - International JournalDocument4 pagesA Case Report of Liver Infiltration From A Large - 2024 - International JournalRonald QuezadaPas encore d'évaluation
- LAPAROSDocument13 pagesLAPAROSpancholin_9Pas encore d'évaluation
- Anesthesiafor Hepatobiliarysurgery: Chris Snowden,, James PrentisDocument17 pagesAnesthesiafor Hepatobiliarysurgery: Chris Snowden,, James PrentisGiovanni AgugginiPas encore d'évaluation
- 10.1007@s00464 019 06670 9Document17 pages10.1007@s00464 019 06670 9Francisco Javier MacíasPas encore d'évaluation
- Articulo 1Document8 pagesArticulo 1Luzmaria CortesPas encore d'évaluation
- Current Opinion On Lymphadenectomy in Pancreatic Cancer SurgeryDocument5 pagesCurrent Opinion On Lymphadenectomy in Pancreatic Cancer Surgeryyacine26Pas encore d'évaluation
- Quistectomía Laparoscópica en Quiste Hidatídico Hepático: Laparoscopic Cystectomy in Hidatidid CystDocument7 pagesQuistectomía Laparoscópica en Quiste Hidatídico Hepático: Laparoscopic Cystectomy in Hidatidid CystIvette AlvarezPas encore d'évaluation
- Laparoscopic Surgery in Gynaecologic OncologyDocument7 pagesLaparoscopic Surgery in Gynaecologic OncologyManan BoobPas encore d'évaluation
- Moussa Et Al. (2021)Document12 pagesMoussa Et Al. (2021)Tere OliverosPas encore d'évaluation
- World Journal of Emergency Surgery: Emergency Laparoscopy - Current Best PracticeDocument9 pagesWorld Journal of Emergency Surgery: Emergency Laparoscopy - Current Best PracticeHendra JojoPas encore d'évaluation
- Zhou2004 Article LaparoscopicVersusOpenTotalMesDocument5 pagesZhou2004 Article LaparoscopicVersusOpenTotalMesWarren SeowPas encore d'évaluation
- Overview of Hepatic ResectionDocument27 pagesOverview of Hepatic Resectionhiwotbetesfa2123Pas encore d'évaluation
- World Journal of Gastroenterology, Hepatology and Endoscopy: Article InformationDocument4 pagesWorld Journal of Gastroenterology, Hepatology and Endoscopy: Article Informationscience world publishingPas encore d'évaluation
- DAnnibale2004 Article RoboticAndLaparoscopicSurgeryFDocument7 pagesDAnnibale2004 Article RoboticAndLaparoscopicSurgeryFWarren SeowPas encore d'évaluation
- Resection of Colorectal Liver Metastases: Ssat/Ahpba Joint Symposium 2010Document4 pagesResection of Colorectal Liver Metastases: Ssat/Ahpba Joint Symposium 2010Nikos SerifisPas encore d'évaluation
- Robotic Total Mesorectal Excision For Low Rectal CancerDocument10 pagesRobotic Total Mesorectal Excision For Low Rectal CancerAnitei GabrielaPas encore d'évaluation
- Figures 1Document8 pagesFigures 1Arman KozhakhmetPas encore d'évaluation
- 02 PDFDocument17 pages02 PDFDrelsayed HagagPas encore d'évaluation
- Annals of Medicine and Surgery: SciencedirectDocument5 pagesAnnals of Medicine and Surgery: SciencedirectilhamPas encore d'évaluation
- Wind2007 PDFDocument5 pagesWind2007 PDFanatolioPas encore d'évaluation
- Timetable PosterExDocument45 pagesTimetable PosterExNeo Rodriguez AlvaradoPas encore d'évaluation
- Fundus First Laparoscopic Cholecystectomy Technique Reduces ComplicationsDocument5 pagesFundus First Laparoscopic Cholecystectomy Technique Reduces ComplicationsRony RonyPas encore d'évaluation
- Vascular Surgery in Liver Resection: Olga Radulova Mauersberger Jürgen Weitz Carina RiedigerDocument32 pagesVascular Surgery in Liver Resection: Olga Radulova Mauersberger Jürgen Weitz Carina RiedigerariPas encore d'évaluation
- Atlas of Anatomic Hepatic Resection For Hepatocellular CarcinomaDocument339 pagesAtlas of Anatomic Hepatic Resection For Hepatocellular CarcinomaValean Dan100% (1)
- Overview of Hepatic Resection Techniques and IndicationsDocument30 pagesOverview of Hepatic Resection Techniques and Indicationsbo gum parkPas encore d'évaluation
- HPB2010 791625Document6 pagesHPB2010 791625ocramusPas encore d'évaluation
- 2023 Article 1954Document6 pages2023 Article 1954davidmarkovic032Pas encore d'évaluation
- Celiac Lymph Node Resection and Porta Hepatis DiseaseDocument6 pagesCeliac Lymph Node Resection and Porta Hepatis DiseaseAndreeaPopescuPas encore d'évaluation
- Colorectal SurgeryDocument73 pagesColorectal SurgeryShashidhara PuttarajPas encore d'évaluation
- Hepatectomy For Hilar Cholangiocarcinoma With RighDocument8 pagesHepatectomy For Hilar Cholangiocarcinoma With RighGolam MahmudPas encore d'évaluation
- Laparoscopic Aproach in Hidatic CystDocument17 pagesLaparoscopic Aproach in Hidatic CystcrisssPas encore d'évaluation
- 0102 6720 Abcd 32 01 E1426Document5 pages0102 6720 Abcd 32 01 E1426Amaury de la CruzPas encore d'évaluation
- 1-s2.0-S2667008923000253-mainDocument4 pages1-s2.0-S2667008923000253-mainal malikPas encore d'évaluation
- COLONDocument24 pagesCOLONYS NatePas encore d'évaluation
- Yamamoto1999 PDFDocument5 pagesYamamoto1999 PDFalexPas encore d'évaluation
- 2015 Laparoscopic Surgery in Abdominal Trauma A Single Center Review of A 7-Year ExperienceDocument7 pages2015 Laparoscopic Surgery in Abdominal Trauma A Single Center Review of A 7-Year ExperiencejohnnhekoPas encore d'évaluation
- Anaesthesia For Hepatic Resection SurgeryDocument15 pagesAnaesthesia For Hepatic Resection SurgeryDianita P Ñáñez VaronaPas encore d'évaluation
- Ehinokok Jetre PDFDocument10 pagesEhinokok Jetre PDFNemanja VukcevicPas encore d'évaluation
- Surgical Techniques For Pancreas Transplantation: Ugo Boggi, Gabriella Amorese and Piero MarchettiDocument10 pagesSurgical Techniques For Pancreas Transplantation: Ugo Boggi, Gabriella Amorese and Piero MarchettiNatalindah Jokiem Woecandra T. D.Pas encore d'évaluation
- Colon Resection For Ovarian CancerDocument10 pagesColon Resection For Ovarian CancerAndreeaPopescuPas encore d'évaluation
- Laparoscopic Cholecystectomy After Conservative Su - 2024 - International JournaDocument4 pagesLaparoscopic Cholecystectomy After Conservative Su - 2024 - International JournaRonald QuezadaPas encore d'évaluation
- Appleby OperationDocument9 pagesAppleby OperationPeter Paul PascualPas encore d'évaluation
- Hino H. Et Al.,2017Document8 pagesHino H. Et Al.,2017Mai M. AlshalPas encore d'évaluation
- Totally Laparoscipic Right Colectomy: Technique Description: Hepato-Gastroenterology April 2015Document5 pagesTotally Laparoscipic Right Colectomy: Technique Description: Hepato-Gastroenterology April 2015anatomPas encore d'évaluation
- Hepatic Veins Ablated Under Vascular ExclusionDocument7 pagesHepatic Veins Ablated Under Vascular ExclusionAndreeaPopescuPas encore d'évaluation
- Chouillard2010 - Vascular Clamping in Liver Surgery - Physiology, Indications and TechniquesDocument12 pagesChouillard2010 - Vascular Clamping in Liver Surgery - Physiology, Indications and TechniqueshoangducnamPas encore d'évaluation
- IntJAppBasicMedRes64237-2646592 072105Document4 pagesIntJAppBasicMedRes64237-2646592 072105hoangducnamPas encore d'évaluation
- Fong1997 - Useful Stapling Techniques in Liver SurgeryDocument8 pagesFong1997 - Useful Stapling Techniques in Liver SurgeryhoangducnamPas encore d'évaluation
- Alvarez2016 - Parenchymal-Sparing Liver Surgery in Patients With Colorectal Carcinoma Liver Metastases PDFDocument18 pagesAlvarez2016 - Parenchymal-Sparing Liver Surgery in Patients With Colorectal Carcinoma Liver Metastases PDFhoangducnamPas encore d'évaluation
- Factor Analysis in SPSSDocument9 pagesFactor Analysis in SPSSLoredana IcsulescuPas encore d'évaluation
- Hepatic Manifestations in Hematological Disorders 2013Document14 pagesHepatic Manifestations in Hematological Disorders 2013hoangducnamPas encore d'évaluation
- Best VideoDocument16 pagesBest VideohoangducnamPas encore d'évaluation
- Helling2014 - Ton That Tung's LiversDocument8 pagesHelling2014 - Ton That Tung's Livershoangducnam100% (1)
- Safety of Donors in Live Donor Liver Transplantation Using Right Lobe Grafts 2014Document5 pagesSafety of Donors in Live Donor Liver Transplantation Using Right Lobe Grafts 2014hoangducnamPas encore d'évaluation
- The Associating Liver Partition and Portal Vein Ligation For Staged Hepatectomy Approach Using Only Segments I and IV As Future Liver RemnantDocument5 pagesThe Associating Liver Partition and Portal Vein Ligation For Staged Hepatectomy Approach Using Only Segments I and IV As Future Liver RemnanthoangducnamPas encore d'évaluation
- Split RevisionDocument13 pagesSplit RevisionhoangducnamPas encore d'évaluation
- Combined Liver-Kidney Transplantation in Patients With Cirrhosis and Chronic Kidney DiseaseDocument8 pagesCombined Liver-Kidney Transplantation in Patients With Cirrhosis and Chronic Kidney DiseasehoangducnamPas encore d'évaluation
- IELTS Listening - Reading Answer SheetsDocument2 pagesIELTS Listening - Reading Answer Sheetsntnam11383% (12)
- IELTS Reading Answer SheetDocument1 pageIELTS Reading Answer Sheetskuppal50% (2)
- Cholangiocarcinoma diagnosis and treatment advancesDocument12 pagesCholangiocarcinoma diagnosis and treatment advanceslimbert manuelPas encore d'évaluation
- Classification, Diagnosis, and Management of Cholangiocarcinoma - Razumilava2013Document10 pagesClassification, Diagnosis, and Management of Cholangiocarcinoma - Razumilava2013hoangducnamPas encore d'évaluation
- Dumortier2016 - EVEROLIMUSDocument10 pagesDumortier2016 - EVEROLIMUShoangducnamPas encore d'évaluation
- SAS BigData FinalDocument37 pagesSAS BigData FinalDevika RadjkoemarPas encore d'évaluation
- Academic Test 1 Question PaperDocument21 pagesAcademic Test 1 Question PaperPeach Peach Lynn0% (2)
- The Lover CompleteDocument18 pagesThe Lover Completehoangducnam100% (1)
- Kaumarbhritya Question BankDocument38 pagesKaumarbhritya Question BankINSTA SHORTSPas encore d'évaluation
- Drug Study Rle G10Document18 pagesDrug Study Rle G10Kirsten Moreen GuevarraPas encore d'évaluation
- A Review of Animal Welfare Protocol On Dog Shelter in Java Area IndonesiaDocument3 pagesA Review of Animal Welfare Protocol On Dog Shelter in Java Area IndonesiaSorin MarkovPas encore d'évaluation
- Caglar H.B. - SBRT For Lung CancerDocument51 pagesCaglar H.B. - SBRT For Lung CancerÖzgür Kara (OncoHealth)Pas encore d'évaluation
- Obstructive Sleep ApneaDocument58 pagesObstructive Sleep ApneaShristi Chahal100% (2)
- 2020 Green Acute and Chronic Pain InjuryDocument4 pages2020 Green Acute and Chronic Pain InjuryRebecca KnightPas encore d'évaluation
- Improving Functional Outcomes in Physical PDFDocument449 pagesImproving Functional Outcomes in Physical PDFBriana Sturgis100% (3)
- Rumination Syndrome: The Forgotten OffenderDocument3 pagesRumination Syndrome: The Forgotten OffenderBoston Science PublishingPas encore d'évaluation
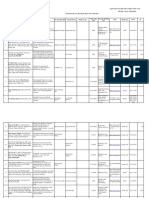
- Pcso Mam Program Services and RequirementsDocument12 pagesPcso Mam Program Services and RequirementsJen UmlanoPas encore d'évaluation
- Danh Sach Bai Bao Quoc Te 2020 794Document14 pagesDanh Sach Bai Bao Quoc Te 2020 794Master DrPas encore d'évaluation
- The PlagueDocument10 pagesThe PlagueChristopher Ceballos Antiporda ɪɪPas encore d'évaluation
- 4 - Assessing EarDocument7 pages4 - Assessing EarFrancine Julia MorilloPas encore d'évaluation
- Cicrulatory and Immune Workbook KEYDocument32 pagesCicrulatory and Immune Workbook KEYgeorgia robinsonPas encore d'évaluation
- Amna Ramzan SKMHDocument36 pagesAmna Ramzan SKMHHAFIZ MUHAMMAD IMTIAZPas encore d'évaluation
- Mitral Stenosis Case PresentationDocument7 pagesMitral Stenosis Case PresentationOM BAWNEPas encore d'évaluation
- Graphites 01 PDFDocument3 pagesGraphites 01 PDFASLAMPas encore d'évaluation
- đề 5Document8 pagesđề 5Chi LêPas encore d'évaluation
- Nursing care for pregnant women with HIVDocument24 pagesNursing care for pregnant women with HIVNithiya NadesanPas encore d'évaluation
- Health Safety and Nutrition For The Young Child 9th Edition Marotz Test BankDocument21 pagesHealth Safety and Nutrition For The Young Child 9th Edition Marotz Test BankJosephWilliamsinaom100% (13)
- Arsenic ToxicityDocument26 pagesArsenic ToxicityDyar MzafarPas encore d'évaluation
- Advanced Electrolysis TechniquesDocument2 pagesAdvanced Electrolysis Techniquesandres mesaPas encore d'évaluation
- UntitledDocument304 pagesUntitledSubhranil MannaPas encore d'évaluation
- Activity 1, 2 - LabDocument9 pagesActivity 1, 2 - LabShemei Ann ManuelPas encore d'évaluation
- Opel Astra J 2016 Electrical Wiring DiagramsDocument22 pagesOpel Astra J 2016 Electrical Wiring Diagramscodyperry250696cgt100% (120)
- Pancreatitis Case StudyDocument11 pagesPancreatitis Case Studysunny kumarPas encore d'évaluation
- Instant Download Ebook PDF Abrams Clinical Drug Therapy Rationales For Nursing Practice 11th Edition PDF ScribdDocument38 pagesInstant Download Ebook PDF Abrams Clinical Drug Therapy Rationales For Nursing Practice 11th Edition PDF Scribdkimberly.davis644100% (41)
- Ajol File Journals - 473 - Articles - 200776 - Submission - Proof - 200776 5581 503678 1 10 20201026Document7 pagesAjol File Journals - 473 - Articles - 200776 - Submission - Proof - 200776 5581 503678 1 10 20201026hammed nurudeenPas encore d'évaluation
- Anabolic SteroidsDocument5 pagesAnabolic SteroidsGideon MurathaPas encore d'évaluation
- Anaesthesia Considerations for Myasthenia Gravis Patients Undergoing ThymectomyDocument11 pagesAnaesthesia Considerations for Myasthenia Gravis Patients Undergoing ThymectomyParvathy RPas encore d'évaluation
- Anthracinum. - THE GUIDING SYMPTOMS OF OUR MATERIA MEDICA by CONSTANTINE HERINGDocument17 pagesAnthracinum. - THE GUIDING SYMPTOMS OF OUR MATERIA MEDICA by CONSTANTINE HERINGHarrison DavidsonPas encore d'évaluation