Vous aimerez peut-être aussi
- Gastric Outlet Obstruction, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsD'EverandGastric Outlet Obstruction, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsPas encore d'évaluation
- Meno Pause&HRTsDocument27 pagesMeno Pause&HRTsMajed AlhuzaliPas encore d'évaluation
- Intrauterine Growth RestrictionDocument3 pagesIntrauterine Growth RestrictionShofiKhaqulIlmyPas encore d'évaluation
- Keehbauch Menopause HRT 4.2.16 SCDocument55 pagesKeehbauch Menopause HRT 4.2.16 SCMuhammad AzkaPas encore d'évaluation
- 9fetal Well Being in PregnancyDocument10 pages9fetal Well Being in PregnancyuouoPas encore d'évaluation
- Intrauterine Growth RestrictionDocument11 pagesIntrauterine Growth Restrictionantonio91uPas encore d'évaluation
- AUB StartedDocument13 pagesAUB StartedIbrahim AbdullahPas encore d'évaluation
- Ovarian Cysts and Cancer in PregnancyDocument15 pagesOvarian Cysts and Cancer in Pregnancykarina100% (1)
- Myop in PregnancyDocument4 pagesMyop in PregnancySamuel WilliamsPas encore d'évaluation
- Anaemia in PregnancyDocument76 pagesAnaemia in PregnancysivaPas encore d'évaluation
- CTG Classification PDFDocument1 pageCTG Classification PDFAkhmad Ikhsan Prafita PutraPas encore d'évaluation
- Postpartum HemorrhageDocument8 pagesPostpartum HemorrhageMazlina MaidinPas encore d'évaluation
- Recurrent Pregnancy LossDocument61 pagesRecurrent Pregnancy LossHerman FiraPas encore d'évaluation
- Pulmonary Disorders in PregnancyDocument49 pagesPulmonary Disorders in PregnancyMara Medina - BorleoPas encore d'évaluation
- 30 - Contracted Pelvis and Cephalopelvic DisproportionDocument28 pages30 - Contracted Pelvis and Cephalopelvic Disproportiondr_asaleh93% (14)
- ACOG Management of Stillbirth PDFDocument14 pagesACOG Management of Stillbirth PDFLêMinhĐứcPas encore d'évaluation
- Breast Abcess PDFDocument4 pagesBreast Abcess PDFponekPas encore d'évaluation
- 1st & 2nd Trimester Pregnancy LossDocument48 pages1st & 2nd Trimester Pregnancy LossAbdullah EssaPas encore d'évaluation
- Placenta PreviaDocument2 pagesPlacenta PreviaAnonymous 0C4OZmRPas encore d'évaluation
- Precociou S Puberty: BY Vishnupriya Ravimohandoss Year-6 Group-1Document31 pagesPrecociou S Puberty: BY Vishnupriya Ravimohandoss Year-6 Group-1Priya RaviPas encore d'évaluation
- PROM SANJIDA FInal 2Document32 pagesPROM SANJIDA FInal 2Saiful islam RonyPas encore d'évaluation
- Expectatant Management of Cesarean Scar Ectopic PregnancyDocument5 pagesExpectatant Management of Cesarean Scar Ectopic PregnancyEricPas encore d'évaluation
- Acute Fatty Liver With PregnancyDocument50 pagesAcute Fatty Liver With PregnancyDr. mohammed100% (1)
- EndometriosisDocument12 pagesEndometriosisYESIPas encore d'évaluation
- Case Presentation CataractDocument19 pagesCase Presentation CataractRani GherePas encore d'évaluation
- Anorectal Malformations: Presented by Khushveer KaurDocument91 pagesAnorectal Malformations: Presented by Khushveer KaurKataria DavinPas encore d'évaluation
- Anaemia in PregnancyDocument28 pagesAnaemia in PregnancyUsman G. HingoroPas encore d'évaluation
- Hypoxic Ischemic EncephalopathyDocument33 pagesHypoxic Ischemic EncephalopathyDr.P.NatarajanPas encore d'évaluation
- AnencephalyDocument5 pagesAnencephalyNabeel RayedPas encore d'évaluation
- Prevention Cervical Cancer4847Document27 pagesPrevention Cervical Cancer4847Lalita Eka Pervita Sari100% (1)
- Endometrial PolypsDocument14 pagesEndometrial PolypsMusaPas encore d'évaluation
- 06 Reducing Perinatal & Neonatal MortalityDocument68 pages06 Reducing Perinatal & Neonatal MortalityrositaPas encore d'évaluation
- Female Genital TuberculosisDocument6 pagesFemale Genital TuberculosisallauddinbarackzaiPas encore d'évaluation
- Hyperprolactinem IaDocument63 pagesHyperprolactinem Iakhadzx100% (2)
- Case Write-Up Obstetrics & Gynaecology Posting SESSION 2021/2022Document25 pagesCase Write-Up Obstetrics & Gynaecology Posting SESSION 2021/2022Luqman MalekPas encore d'évaluation
- Birth AsphyxiaDocument26 pagesBirth Asphyxiawizborrlyzo006Pas encore d'évaluation
- Epilepsy in Pregnancy JatuDocument57 pagesEpilepsy in Pregnancy Jatuninjahattori1Pas encore d'évaluation
- Scaohoid Fracture 4Document34 pagesScaohoid Fracture 4Noor Al Zahraa Ali100% (1)
- Type B (Hib) Vaccine: Haemophilus InfluenzaeDocument2 pagesType B (Hib) Vaccine: Haemophilus InfluenzaeEnce MalatambanPas encore d'évaluation
- Pre-Eclampsia, Eclampsia and HELLP SyndromeDocument15 pagesPre-Eclampsia, Eclampsia and HELLP SyndromehendraPas encore d'évaluation
- Puerpera L Mental DisordersDocument13 pagesPuerpera L Mental DisordersclarheenaPas encore d'évaluation
- Infertilityseminarppt 190718134710Document77 pagesInfertilityseminarppt 190718134710subiPas encore d'évaluation
- Pregnant Abdomen ExamDocument4 pagesPregnant Abdomen ExamAmiel Francisco ReyesPas encore d'évaluation
- Obg - 9.4.20 (Forenoon) Unit 12 - Infertility and Its ManagementDocument81 pagesObg - 9.4.20 (Forenoon) Unit 12 - Infertility and Its ManagementElakkiyaanu64 Elakkiyaanu64Pas encore d'évaluation
- Salpingo OophorectomyDocument2 pagesSalpingo OophorectomyKasamapon Oak ChawanachitPas encore d'évaluation
- Approach To The Patient With An Adnexal Mass - UpToDateDocument31 pagesApproach To The Patient With An Adnexal Mass - UpToDateRamackPas encore d'évaluation
- Hypertension in PregnancyDocument45 pagesHypertension in PregnancyMary Anne Cabalza ApinardoPas encore d'évaluation
- Changing Trends in Cesarean DeliveryDocument7 pagesChanging Trends in Cesarean DeliveryEditor_IAIMPas encore d'évaluation
- Per Vaginal Bleeding in PregnancyDocument33 pagesPer Vaginal Bleeding in PregnancyKai Wei LimPas encore d'évaluation
- Hypertension in PregnancyDocument68 pagesHypertension in PregnancyAbdul MoizPas encore d'évaluation
- Cervical Incompetence Moh AbdallaDocument46 pagesCervical Incompetence Moh AbdallaDr. mohammed50% (2)
- Early Pregnancy LossDocument20 pagesEarly Pregnancy LossRima HajjarPas encore d'évaluation
- Intrauterine Contraception: Copper T 380A (Paragard®) Levonorgestrel-Releasing Intrauterine System (Mirena®)Document16 pagesIntrauterine Contraception: Copper T 380A (Paragard®) Levonorgestrel-Releasing Intrauterine System (Mirena®)Fia Delfia AdventyPas encore d'évaluation
- Newest Cervical CancerDocument14 pagesNewest Cervical CancerSAMMYPas encore d'évaluation
- High Risk PregnancyDocument44 pagesHigh Risk PregnancyKavipriyaPas encore d'évaluation
- HepatitisDocument3 pagesHepatitisElieth ConcepciónPas encore d'évaluation
- Immunological Causes of Bad Obstetric HistoryDocument14 pagesImmunological Causes of Bad Obstetric HistoryDara Dasawulansari SyamsuriPas encore d'évaluation
- Antiphospholipid Antibody Syndrome and PregnancyDocument7 pagesAntiphospholipid Antibody Syndrome and PregnancystepepsPas encore d'évaluation
- Reproductive ImmunologyDocument3 pagesReproductive Immunologymohd_ikrayemPas encore d'évaluation
- RPL2 ReportDocument66 pagesRPL2 ReportJoseph DavidPas encore d'évaluation
- Jurnal Reading RiwDocument33 pagesJurnal Reading RiwRiyan W. PratamaPas encore d'évaluation
- Duty Report 5.12.1978Document55 pagesDuty Report 5.12.1978Riyan W. PratamaPas encore d'évaluation
- Book Reading-Cervical InsufficiencyDocument32 pagesBook Reading-Cervical InsufficiencyRiyan W. PratamaPas encore d'évaluation
- Duty Report IIIDocument8 pagesDuty Report IIIRiyan W. PratamaPas encore d'évaluation
- Duty Report RIWDocument41 pagesDuty Report RIWRiyan W. PratamaPas encore d'évaluation
- Duty Report 5.12.1978Document55 pagesDuty Report 5.12.1978Riyan W. PratamaPas encore d'évaluation
- Duty Report "Example"Document9 pagesDuty Report "Example"Riyan W. PratamaPas encore d'évaluation
- Duty Report "Example"Document9 pagesDuty Report "Example"Riyan W. PratamaPas encore d'évaluation
- Obstetric Outpatient: Monday, April 2 2018Document2 pagesObstetric Outpatient: Monday, April 2 2018Riyan W. PratamaPas encore d'évaluation
- Effect of Ibuprofen Vs Acetaminophen On Postpartum Hypertension in Preeclampsia With Severe Features: A Double-Masked, Randomized Controlled TrialDocument24 pagesEffect of Ibuprofen Vs Acetaminophen On Postpartum Hypertension in Preeclampsia With Severe Features: A Double-Masked, Randomized Controlled TrialRiyan W. PratamaPas encore d'évaluation
- Obstetric Outpatient: Friday, April 20 2018Document14 pagesObstetric Outpatient: Friday, April 20 2018Riyan W. PratamaPas encore d'évaluation
- Obstetric Outpatient: Wednesday, April 4 2018Document9 pagesObstetric Outpatient: Wednesday, April 4 2018Riyan W. PratamaPas encore d'évaluation
- Obstetric Outpatient: Monday, April 2 2018Document22 pagesObstetric Outpatient: Monday, April 2 2018Riyan W. PratamaPas encore d'évaluation
- Fragx SyndromeDocument3 pagesFragx SyndromeRiyan W. PratamaPas encore d'évaluation
- Associate-Shopping in Hyderabad, Telangana Careers at HyderabadDocument1 pageAssociate-Shopping in Hyderabad, Telangana Careers at HyderabadpavanPas encore d'évaluation
- Letters of ComplaintDocument3 pagesLetters of ComplaintMercedes Jimenez RomanPas encore d'évaluation
- LRL Rudy Acuna On Neftali DeLeon - I Am Proud To Be The Grandson Son and Husband of Immigrants.Document9 pagesLRL Rudy Acuna On Neftali DeLeon - I Am Proud To Be The Grandson Son and Husband of Immigrants.EditorPas encore d'évaluation
- Live Leak - SSC CGL Tier II English Model Question Paper (Based On Predicted Pattern 2016)Document44 pagesLive Leak - SSC CGL Tier II English Model Question Paper (Based On Predicted Pattern 2016)Testbook BlogPas encore d'évaluation
- Reaction PaperDocument3 pagesReaction PaperPatrick Ramos80% (15)
- Simple Past Story 1Document7 pagesSimple Past Story 1Ummi Umarah50% (2)
- By Nur Fatin Najihah Binti NoruddinDocument7 pagesBy Nur Fatin Najihah Binti NoruddinNajihah NoruddinPas encore d'évaluation
- 1 Patient Assessment Form.Document3 pages1 Patient Assessment Form.Aina HaravataPas encore d'évaluation
- Logical Remarks On The Semantic Approach PDFDocument34 pagesLogical Remarks On The Semantic Approach PDFFelipe SantosPas encore d'évaluation
- Concept of Leadership (Session-1) MARSDocument14 pagesConcept of Leadership (Session-1) MARShudaPas encore d'évaluation
- Guoyin Shen, Ho-Kwang Mao and Russell J. Hemley - Laser-Heated Diamond Anvil Cell Technique: Double-Sided Heating With Multimode Nd:YAG LaserDocument5 pagesGuoyin Shen, Ho-Kwang Mao and Russell J. Hemley - Laser-Heated Diamond Anvil Cell Technique: Double-Sided Heating With Multimode Nd:YAG LaserDeez34PPas encore d'évaluation
- I. Title: "REPAINTING: Streetlight Caution Signs"Document5 pagesI. Title: "REPAINTING: Streetlight Caution Signs"Ziegfred AlmontePas encore d'évaluation
- Icmap Newsletter June 2017Document7 pagesIcmap Newsletter June 2017GoopPas encore d'évaluation
- Inheritance : Trung Tâm Anh NG Nhung PH M 27N7A KĐT Trung Hòa Nhân Chính - 0946 530 486 - 0964 177 322Document3 pagesInheritance : Trung Tâm Anh NG Nhung PH M 27N7A KĐT Trung Hòa Nhân Chính - 0946 530 486 - 0964 177 322Trung PhamPas encore d'évaluation
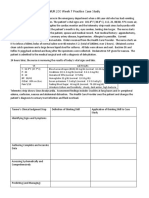
- NUR 200 Week 7 Practice Case StudyDocument2 pagesNUR 200 Week 7 Practice Case StudyJB NicolePas encore d'évaluation
- Consti II Case ListDocument44 pagesConsti II Case ListGeron Gabriell SisonPas encore d'évaluation
- Project Report: Eveplus Web PortalDocument47 pagesProject Report: Eveplus Web Portaljas121Pas encore d'évaluation
- Gesture and Speech Andre Leroi-GourhanDocument451 pagesGesture and Speech Andre Leroi-GourhanFerda Nur Demirci100% (2)
- PublicadministrationinthephilippinesDocument29 pagesPublicadministrationinthephilippinesGorby ResuelloPas encore d'évaluation
- Year 8 - Higher - Autumn 2019Document16 pagesYear 8 - Higher - Autumn 2019nooraPas encore d'évaluation
- A Social Movement, Based On Evidence, To Reduce Inequalities in Health Michael Marmot, Jessica Allen, Peter GoldblattDocument5 pagesA Social Movement, Based On Evidence, To Reduce Inequalities in Health Michael Marmot, Jessica Allen, Peter GoldblattAmory JimenezPas encore d'évaluation
- Happiness Portrayal and Level of Self-Efficacy Among Public Elementary School Heads in A DivisionDocument13 pagesHappiness Portrayal and Level of Self-Efficacy Among Public Elementary School Heads in A DivisionPsychology and Education: A Multidisciplinary JournalPas encore d'évaluation
- Privileged Communications Between Husband and Wife - Extension of PDFDocument7 pagesPrivileged Communications Between Husband and Wife - Extension of PDFKitingPadayhagPas encore d'évaluation
- Rules of SyllogismDocument6 pagesRules of Syllogismassume5Pas encore d'évaluation
- Elc650 Ws Guidelines (250219)Document3 pagesElc650 Ws Guidelines (250219)panda_yien100% (1)
- Managing Individual Differences and BehaviorDocument40 pagesManaging Individual Differences and BehaviorDyg Norjuliani100% (1)
- Birth Control Comparison Chart 2018Document1 pageBirth Control Comparison Chart 2018Eric SandesPas encore d'évaluation
- BTS WORLD-Crafting GuideDocument4 pagesBTS WORLD-Crafting GuideAn ARMYPas encore d'évaluation
- Deborah Schiffrin .Tense Variation in NarrativeDocument19 pagesDeborah Schiffrin .Tense Variation in Narrativealwan61Pas encore d'évaluation
- 145class 7 Integers CH 1Document2 pages145class 7 Integers CH 17A04Aditya MayankPas encore d'évaluation