Vous aimerez peut-être aussi
- Stealth Adapted Viruses; Alternative Cellular Energy (Ace) & Kelea Activated Water: A New Paradigm of HealthcareD'EverandStealth Adapted Viruses; Alternative Cellular Energy (Ace) & Kelea Activated Water: A New Paradigm of HealthcarePas encore d'évaluation
- Secondary HypertensionD'EverandSecondary HypertensionAlberto MorgantiPas encore d'évaluation
- Infective Endocarditis: Indian Scenario: Rajeev GuptaDocument7 pagesInfective Endocarditis: Indian Scenario: Rajeev GuptapreetPas encore d'évaluation
- Infective EndocarditisDocument18 pagesInfective EndocarditisLee Foo WengPas encore d'évaluation
- Infectious EndocarditisDocument49 pagesInfectious EndocarditisDennisFrankKondoPas encore d'évaluation
- 325 FullDocument20 pages325 FullDessyadoePas encore d'évaluation
- Infective EndocarditisDocument16 pagesInfective EndocarditisAnnisa UlfaPas encore d'évaluation
- Endocarditis Nature 1Document13 pagesEndocarditis Nature 1NAREN FAVIAN BRAVO BRAVOPas encore d'évaluation
- CO - Endocarditis in Critically Ill PatientsDocument8 pagesCO - Endocarditis in Critically Ill PatientsRomán Wagner Thomas Esteli ChávezPas encore d'évaluation
- ENDOCARDITISDocument4 pagesENDOCARDITISrnsharmasPas encore d'évaluation
- DR Bragg - Endocarditis - Pediatric in Review April 2014Document9 pagesDR Bragg - Endocarditis - Pediatric in Review April 2014angelicaPas encore d'évaluation
- Moreillon2004 PDFDocument11 pagesMoreillon2004 PDFMery Luz RojasPas encore d'évaluation
- Infective EndocarditisDocument67 pagesInfective EndocarditisDr. Rajesh PadhiPas encore d'évaluation
- 01 Cir 98 25 2936Document13 pages01 Cir 98 25 2936Ikhsan Amadea9969Pas encore d'évaluation
- Infective Endocarditis: Dwi Ariyanti, MD (Fiha) Fakultas Kedokteran Universitas Jember 2016Document34 pagesInfective Endocarditis: Dwi Ariyanti, MD (Fiha) Fakultas Kedokteran Universitas Jember 2016Aji rahmat HidayahPas encore d'évaluation
- 10 1016@j Mayocp 2019 12 008 PDFDocument16 pages10 1016@j Mayocp 2019 12 008 PDFfadmayulianiPas encore d'évaluation
- Acute Ischaemic Stroke in Infective Endocarditis: Pathophysiology and Clinical Outcomes in Patients Treated With Reperfusion TherapyDocument13 pagesAcute Ischaemic Stroke in Infective Endocarditis: Pathophysiology and Clinical Outcomes in Patients Treated With Reperfusion TherapyPatrick NunsioPas encore d'évaluation
- Infective Endocarditis: Ainal Fadly Adigama PF Enny SuryantiDocument50 pagesInfective Endocarditis: Ainal Fadly Adigama PF Enny SuryantiFaisal Reza AdiebPas encore d'évaluation
- Infective Endocarditis-Update For The Perioperative ClinicianDocument13 pagesInfective Endocarditis-Update For The Perioperative ClinicianMiguel PugaPas encore d'évaluation
- Infective Endocarditis PDFDocument6 pagesInfective Endocarditis PDFMaya WijayaPas encore d'évaluation
- Infective Endocarditis (Ie) : Mengist Awoke (MSC, Assistant Professor)Document29 pagesInfective Endocarditis (Ie) : Mengist Awoke (MSC, Assistant Professor)Digafe TolaPas encore d'évaluation
- 2020 Article 435Document25 pages2020 Article 435Carlos Peña PaterninaPas encore d'évaluation
- Endocarditis Pediatric in ReviewDocument9 pagesEndocarditis Pediatric in ReviewAngela LópezPas encore d'évaluation
- Infective Endocarditis and Dental Procedures: Evidence, Pathogenesis, and PreventionDocument10 pagesInfective Endocarditis and Dental Procedures: Evidence, Pathogenesis, and PreventionSarah Ariefah SantriPas encore d'évaluation
- Infective Endocarditis: A Contemporary Update: Authors: Ronak RajaniDocument5 pagesInfective Endocarditis: A Contemporary Update: Authors: Ronak RajanicositaamorPas encore d'évaluation
- Bacterial EndocarditisDocument14 pagesBacterial EndocarditisSubhanAnwarKhanPas encore d'évaluation
- Native-Valve Infective Endocarditis: Clinical PracticeDocument10 pagesNative-Valve Infective Endocarditis: Clinical PracticeRaul DoctoPas encore d'évaluation
- Aneurism A Aorta InfectadoDocument6 pagesAneurism A Aorta InfectadoYgor AlbuquerquePas encore d'évaluation
- E000174 Full PDFDocument9 pagesE000174 Full PDFRicardo Costa da SilvaPas encore d'évaluation
- 1882-Article Text-7722-1-10-20200608 PDFDocument6 pages1882-Article Text-7722-1-10-20200608 PDFRyanPas encore d'évaluation
- Infective Endocarditis Today (Version 1 Peer Review: 1 Not Approved)Document9 pagesInfective Endocarditis Today (Version 1 Peer Review: 1 Not Approved)preetPas encore d'évaluation
- Sepsis Therapies: Learning From 30 Years of Failure of Translational Research To Propose New LeadsDocument24 pagesSepsis Therapies: Learning From 30 Years of Failure of Translational Research To Propose New LeadsMark TomPas encore d'évaluation
- Pathogens: Nosocomial Infections: Do Not Forget The Parasites!Document22 pagesPathogens: Nosocomial Infections: Do Not Forget The Parasites!lee suk moPas encore d'évaluation
- Seminar - Infective EndocarditisDocument12 pagesSeminar - Infective EndocarditisJorge Chavez100% (1)
- Endocard BartonDocument4 pagesEndocard BartonKrull TTTeamPas encore d'évaluation
- Infective EndocarditisDocument68 pagesInfective EndocarditisDr. Rajesh PadhiPas encore d'évaluation
- Adults 5Document5 pagesAdults 5Bshara SleemPas encore d'évaluation
- Diagnostic and Terapi in Infection in Solid TransplantDocument19 pagesDiagnostic and Terapi in Infection in Solid TransplantretnoPas encore d'évaluation
- CASE STUDY - Infective EndocarditisDocument6 pagesCASE STUDY - Infective EndocarditisDudil GoatPas encore d'évaluation
- Pathology and Pathogenesis of Infective Endocarditis in Native Heart ValvesDocument8 pagesPathology and Pathogenesis of Infective Endocarditis in Native Heart ValvesIrina TănasePas encore d'évaluation
- Use Only: Sepsis: Implication For NursingDocument4 pagesUse Only: Sepsis: Implication For NursingDeo RizkyandriPas encore d'évaluation
- Disease of Endocardium, Myocardium and PericardiumDocument54 pagesDisease of Endocardium, Myocardium and PericardiumadystiPas encore d'évaluation
- Infective Endocarditis Case ReportDocument40 pagesInfective Endocarditis Case Reportliu_owen17100% (1)
- Wu Et Al 2017 - Epidemiology and Risk Factors of Infective Endocarditis in Children in ChinaDocument10 pagesWu Et Al 2017 - Epidemiology and Risk Factors of Infective Endocarditis in Children in ChinaOktadoni SaputraPas encore d'évaluation
- Endocarditis in The Intensive Care Unit An UpdateDocument10 pagesEndocarditis in The Intensive Care Unit An Updatecarper454Pas encore d'évaluation
- Infective Endocarditis AbnetDocument198 pagesInfective Endocarditis AbnetAbnet WondimuPas encore d'évaluation
- Report EndocarditisDocument38 pagesReport EndocarditisCamille MarasiganPas encore d'évaluation
- Cardiac EmergenciesDocument21 pagesCardiac Emergenciesgus_lionsPas encore d'évaluation
- EndocarditisDocument53 pagesEndocarditisمحمد ربيعيPas encore d'évaluation
- Sbe in ChildrenDocument42 pagesSbe in Childrengrim reaperPas encore d'évaluation
- Lecture Infective EndocarditisDocument37 pagesLecture Infective EndocarditisJohnson OlawalePas encore d'évaluation
- AaaaDocument57 pagesAaaaandreva8Pas encore d'évaluation
- Myocarditis: Leslie T. Cooper Jr. and Kirk U. KnowltonDocument21 pagesMyocarditis: Leslie T. Cooper Jr. and Kirk U. KnowltonAnonymous cdLyeXKBPas encore d'évaluation
- 2022 Pathogenesis, Diagnosis, Antimicrobial Therapy and Management of Infective Endocarditis, and Its ComplicationsDocument7 pages2022 Pathogenesis, Diagnosis, Antimicrobial Therapy and Management of Infective Endocarditis, and Its ComplicationsstedorasPas encore d'évaluation
- Human Immunodeficiency Virus: Anesthetic and Obstetric ConsiderationsDocument9 pagesHuman Immunodeficiency Virus: Anesthetic and Obstetric ConsiderationsNani OktaviaPas encore d'évaluation
- Acute Kidney Injury1Document16 pagesAcute Kidney Injury1Hmn07Pas encore d'évaluation
- Frenemies Within: An Endocarditis Case in Behçet's DiseaseDocument12 pagesFrenemies Within: An Endocarditis Case in Behçet's DiseaseCatherine MorrisPas encore d'évaluation
- JTD 11 01 21Document8 pagesJTD 11 01 21Kornelis AribowoPas encore d'évaluation
- Infective Endocarditis: Update On Epidemiology, Outcomes, and ManagementDocument9 pagesInfective Endocarditis: Update On Epidemiology, Outcomes, and ManagementRaul Cesar Solis EndaraPas encore d'évaluation
- Auto-Inflammatory Syndromes: Pathophysiology, Diagnosis, and ManagementD'EverandAuto-Inflammatory Syndromes: Pathophysiology, Diagnosis, and ManagementPetros EfthimiouPas encore d'évaluation
- The Analysis and Reflection On That Sugar FilmDocument2 pagesThe Analysis and Reflection On That Sugar FilmkkkkPas encore d'évaluation
- Breast Imaging Review - A Quick Guide To Essential Diagnoses (2nd Edition) PDFDocument264 pagesBreast Imaging Review - A Quick Guide To Essential Diagnoses (2nd Edition) PDFGregorio Parra100% (2)
- Adult Early Warning Score Observation Chart For Cardiothoracic UnitDocument1 pageAdult Early Warning Score Observation Chart For Cardiothoracic UnitalexipsPas encore d'évaluation
- NCPDocument14 pagesNCPclaidelynPas encore d'évaluation
- SCIT 1408 Applied Human Anatomy and Physiology II - Urinary System Chapter 25 BDocument50 pagesSCIT 1408 Applied Human Anatomy and Physiology II - Urinary System Chapter 25 BChuongPas encore d'évaluation
- ERCPDocument4 pagesERCPbilly wilsonPas encore d'évaluation
- DSM OcdDocument2 pagesDSM Ocdnmyza89Pas encore d'évaluation
- Complications of DiabetesDocument3 pagesComplications of Diabetesa7wfPas encore d'évaluation
- Ironfang Invasion - Players GuideDocument12 pagesIronfang Invasion - Players GuideThomas McDonaldPas encore d'évaluation
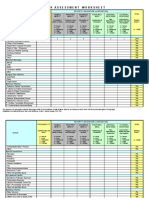
- IC Risk Assessment Worksheet - Kangas-V2.1-Aug.2010 1Document4 pagesIC Risk Assessment Worksheet - Kangas-V2.1-Aug.2010 1Juon Vairzya AnggraeniPas encore d'évaluation
- Histopathology of Dental CariesDocument7 pagesHistopathology of Dental CariesJOHN HAROLD CABRADILLAPas encore d'évaluation
- Kelseys ResumeDocument1 pageKelseys Resumeapi-401573835Pas encore d'évaluation
- The Nadi Vigyan by DR - Sharda Mishra MD (Proff. in Jabalpur Ayurved College)Document5 pagesThe Nadi Vigyan by DR - Sharda Mishra MD (Proff. in Jabalpur Ayurved College)Vivek PandeyPas encore d'évaluation
- ACR-Global Hand Washing Day 2021Document2 pagesACR-Global Hand Washing Day 2021Katy Chenee Napao Perez100% (1)
- Tumor Marker Tests - CancerDocument4 pagesTumor Marker Tests - CancerMonna Medani LysabellaPas encore d'évaluation
- ResearchDocument28 pagesResearchReylon PachesPas encore d'évaluation
- 13) Technical Guideline On Irritation, Sensitization and Hemolysis Study For Chemical DrugsDocument36 pages13) Technical Guideline On Irritation, Sensitization and Hemolysis Study For Chemical DrugsAzam DanishPas encore d'évaluation
- Criminal SociologyDocument53 pagesCriminal SociologyJackielyn cabayaoPas encore d'évaluation
- Nursing Care of The Client With High-Risk Labor & DeliveryDocument10 pagesNursing Care of The Client With High-Risk Labor & DeliveryWilbert CabanbanPas encore d'évaluation
- 3yc CrVlEemddAqBQMk Og 1.4 Six Artifacts From The Future of Food IFTF Coursera 2019Document13 pages3yc CrVlEemddAqBQMk Og 1.4 Six Artifacts From The Future of Food IFTF Coursera 2019Omar YussryPas encore d'évaluation
- Beauty Care 1st Summative TestDocument4 pagesBeauty Care 1st Summative TestLlemor Soled SeyerPas encore d'évaluation
- Tes TLMDocument16 pagesTes TLMAmelia RosyidaPas encore d'évaluation
- Tamiflu and ADHDDocument10 pagesTamiflu and ADHDlaboewe100% (2)
- BELIZARIO VY Et Al Medical Parasitology in The Philippines 3e 158 226Document69 pagesBELIZARIO VY Et Al Medical Parasitology in The Philippines 3e 158 226Sharon Agor100% (1)
- Five Elements Chart TableDocument7 pagesFive Elements Chart TablePawanPas encore d'évaluation
- Zoology MCQs Practice Test 19Document4 pagesZoology MCQs Practice Test 19Rehan HaiderPas encore d'évaluation
- Physiology of The Cell: H. Khorrami PH.DDocument89 pagesPhysiology of The Cell: H. Khorrami PH.Dkhorrami4Pas encore d'évaluation
- Sample Chapter of Assessment Made Incredibly Easy! 1st UK EditionDocument28 pagesSample Chapter of Assessment Made Incredibly Easy! 1st UK EditionLippincott Williams and Wilkins- Europe100% (1)
- Nclex Mnemonics 2020 2Document9 pagesNclex Mnemonics 2020 2Winnie OkothPas encore d'évaluation
- Eaves Nickolas A 201211 MASc ThesisDocument69 pagesEaves Nickolas A 201211 MASc Thesisrajeev50588Pas encore d'évaluation