Vous aimerez peut-être aussi
- Final ENT Exam 2011 Class of 07Document8 pagesFinal ENT Exam 2011 Class of 07John M. HemsworthPas encore d'évaluation
- Bailey Reading Ch7 21-50 ArpanDocument61 pagesBailey Reading Ch7 21-50 ArpandeniadillaPas encore d'évaluation
- MCQsDocument13 pagesMCQsVinay BhatPas encore d'évaluation
- Nasopharyngeal Carcinoma Treatment OptionsDocument42 pagesNasopharyngeal Carcinoma Treatment Optionsrama mandelaPas encore d'évaluation
- OrbitDocument59 pagesOrbitapi-3699330Pas encore d'évaluation
- Ent MCQ 1Document17 pagesEnt MCQ 1sushil466Pas encore d'évaluation
- ENT MCQs 2 No KeyDocument7 pagesENT MCQs 2 No Keyadham bani younesPas encore d'évaluation
- Ent PrelimsDocument8 pagesEnt Prelims胡民星Pas encore d'évaluation
- Neet ENTDocument391 pagesNeet ENTwilliamsjoseff0Pas encore d'évaluation
- 3 RfajDocument81 pages3 RfajSheikhaPas encore d'évaluation
- ENT MCQ (Not Answered)Document75 pagesENT MCQ (Not Answered)mohamed mowafeyPas encore d'évaluation
- ENT MCQs Basic 13Qs.Document5 pagesENT MCQs Basic 13Qs.adham bani younesPas encore d'évaluation
- Ent NotesDocument3 pagesEnt Notesapi-26186766Pas encore d'évaluation
- Ent LQ1Document41 pagesEnt LQ1Raven CocjinPas encore d'évaluation
- Guide to the intercollegiate MRCS (ENT) examDocument18 pagesGuide to the intercollegiate MRCS (ENT) exammonirul islam shohanPas encore d'évaluation
- Head and Neck Surgery QDocument6 pagesHead and Neck Surgery Qمحمد حميدانPas encore d'évaluation
- Ent Practical Examinations Slides For StudyDocument31 pagesEnt Practical Examinations Slides For StudyMuhdZaeedPas encore d'évaluation
- Chhabhadiya Laxman (Ent)Document7 pagesChhabhadiya Laxman (Ent)Venkatesh GarikapatiPas encore d'évaluation
- ENT MCQforstudents AnswersDocument30 pagesENT MCQforstudents AnswersOlaPas encore d'évaluation
- Multiple Choices Questions For ENT ResidentsDocument5 pagesMultiple Choices Questions For ENT Residentsadham bani younesPas encore d'évaluation
- Sudden Sensorineural Hearing Loss: Hou-Yong KangDocument12 pagesSudden Sensorineural Hearing Loss: Hou-Yong KangsuciPas encore d'évaluation
- Ent TestDocument5 pagesEnt TestJohn M. HemsworthPas encore d'évaluation
- ENT MCQs Eiad NahlaDocument11 pagesENT MCQs Eiad Nahlaadham bani younesPas encore d'évaluation
- ENT Best Answer Select The One Best Answer:-: Omdurman Islamic University Medical Students AssociationDocument22 pagesENT Best Answer Select The One Best Answer:-: Omdurman Islamic University Medical Students AssociationAbd AlsalihiPas encore d'évaluation
- Ent AnaDocument79 pagesEnt AnaGyanendra KumarPas encore d'évaluation
- Intercollegiate Specialty Exam in ENT RegulationsDocument4 pagesIntercollegiate Specialty Exam in ENT RegulationsDr-Firas Nayf Al-ThawabiaPas encore d'évaluation
- (ENT-OPT-FRS) End-Posting Examination Questions (G5) - 20180208 - 175513Document23 pages(ENT-OPT-FRS) End-Posting Examination Questions (G5) - 20180208 - 175513Steph StephaniePas encore d'évaluation
- Ent Bcqs 3Document18 pagesEnt Bcqs 3Ghazi Uddin Ahmed0% (1)
- Otorhinolaryngology (ENT) Syllabus of ENT 4 and 6 Semester EARDocument10 pagesOtorhinolaryngology (ENT) Syllabus of ENT 4 and 6 Semester EARShubhashish SinghathakurPas encore d'évaluation
- ENT MneumonicDocument4 pagesENT MneumonicVolksWongsathornPas encore d'évaluation
- Chemoprevention Head Neck MalignanciesDocument3 pagesChemoprevention Head Neck MalignanciesSuprit Sn100% (2)
- Second and Third Year Ent McqsDocument6 pagesSecond and Third Year Ent Mcqsadham bani younesPas encore d'évaluation
- Q. P. Code: 524072Document17 pagesQ. P. Code: 524072Gajzender Singh RanaPas encore d'évaluation
- MCQ It Blok 19 2006Document15 pagesMCQ It Blok 19 2006Anonymous XuDFuevOxPas encore d'évaluation
- ENT Emergency PresentationDocument135 pagesENT Emergency PresentationshahiruddinPas encore d'évaluation
- امتحان ENT دفعة ٣١Document14 pagesامتحان ENT دفعة ٣١محمد عبد القاهر السروريPas encore d'évaluation
- Acute Suppurative Otitis MediaDocument87 pagesAcute Suppurative Otitis MediaHermawan Surya Dharma100% (1)
- Benign and Malignant Neoplasia of URTDocument48 pagesBenign and Malignant Neoplasia of URTsahirbulePas encore d'évaluation
- Questions and Answers Form 1Document33 pagesQuestions and Answers Form 1ahmedPas encore d'évaluation
- 1-The Eustachian Tube Is Opened by Contraction ofDocument10 pages1-The Eustachian Tube Is Opened by Contraction ofNofouz MaswadaPas encore d'évaluation
- Branchial Cleft CystsDocument8 pagesBranchial Cleft CystsHere LeafsPas encore d'évaluation
- E.N.T-Otorhinolaryngology Clerkship Instructions: Read Each Question Carefully and Then Select The Single Best Answer Part I: Otology/EarDocument2 pagesE.N.T-Otorhinolaryngology Clerkship Instructions: Read Each Question Carefully and Then Select The Single Best Answer Part I: Otology/EarJohn M. HemsworthPas encore d'évaluation
- ENT Teams A4 PDFDocument288 pagesENT Teams A4 PDFEbrahim JuniorPas encore d'évaluation
- A. It Consists of Squamous EpitheliumDocument7 pagesA. It Consists of Squamous EpitheliumUzair KhanPas encore d'évaluation
- MCQ KhaldounDocument9 pagesMCQ Khaldounadham bani younesPas encore d'évaluation
- Endocrine DisordersDocument51 pagesEndocrine DisordersavisenicPas encore d'évaluation
- MCQZDocument55 pagesMCQZyasinoPas encore d'évaluation
- Candidate Instructions and Guidance NotesDocument5 pagesCandidate Instructions and Guidance NotesShaun DaveyPas encore d'évaluation
- Family Physicians Guide to ENT ProblemsDocument15 pagesFamily Physicians Guide to ENT ProblemsVitorLópezPas encore d'évaluation
- 4 Dohns May 2004Document7 pages4 Dohns May 2004rizwan afzalPas encore d'évaluation
- Assessing Ear Pain in ChildrenDocument20 pagesAssessing Ear Pain in ChildrenPrince K. TaileyPas encore d'évaluation
- ENT EmergencyDocument57 pagesENT EmergencykylieverPas encore d'évaluation
- EennttDocument13 pagesEennttSuresh Kumar BansalPas encore d'évaluation
- Nasal Polyps: Causes, Symptoms and TreatmentDocument3 pagesNasal Polyps: Causes, Symptoms and TreatmentPuteri Atiqah SyaqilaPas encore d'évaluation
- 1251-1260 MCQ in Facial Plastic and Reconstructive SurgeryDocument8 pages1251-1260 MCQ in Facial Plastic and Reconstructive SurgerySajag GuptaPas encore d'évaluation
- ERMP 2021, Part II-1Document16 pagesERMP 2021, Part II-1kude kulayePas encore d'évaluation
- 100 MCQsDocument35 pages100 MCQsBader AlMajedPas encore d'évaluation
- An Evidence-Based Approach to the Management of Nasopharyngeal Cancer: From Basic Science to Clinical Presentation and TreatmentD'EverandAn Evidence-Based Approach to the Management of Nasopharyngeal Cancer: From Basic Science to Clinical Presentation and TreatmentBaharudin AbdullahPas encore d'évaluation
- Anterior Pharyngeal PouchDocument4 pagesAnterior Pharyngeal PouchGiovanni HenryPas encore d'évaluation
- Reirradiation Meta Analysis and Systematic ReviewDocument13 pagesReirradiation Meta Analysis and Systematic ReviewGiovanni HenryPas encore d'évaluation
- Tracheal StenosisDocument5 pagesTracheal StenosisGiovanni HenryPas encore d'évaluation
- Defining Physiology: Principles, Themes, Concepts.: Hwee Ming Cheng Kin Kheong Mah Kumar SeluakumaranDocument104 pagesDefining Physiology: Principles, Themes, Concepts.: Hwee Ming Cheng Kin Kheong Mah Kumar SeluakumaranGiovanni HenryPas encore d'évaluation
- Recalls of Paper 2 - 11/9/2018: ConsentDocument6 pagesRecalls of Paper 2 - 11/9/2018: ConsentGiovanni Henry0% (1)
- Paediatric Neck MassesDocument7 pagesPaediatric Neck MassesGiovanni HenryPas encore d'évaluation
- Evaluation of The Dizzy PatientDocument61 pagesEvaluation of The Dizzy PatientGiovanni HenryPas encore d'évaluation
- 2018 Cardiovascular PhysiologyDocument197 pages2018 Cardiovascular PhysiologyGladys ParedesPas encore d'évaluation
- Endoscopic Sinus SurgeryDocument91 pagesEndoscopic Sinus SurgeryGiovanni HenryPas encore d'évaluation
- Clinical Features of Ramsay Hunt Syndrome.: C J Sweeney, and D H Gilden J Neurol Neurosurg Psychiatry 2001 71:149-154Document1 pageClinical Features of Ramsay Hunt Syndrome.: C J Sweeney, and D H Gilden J Neurol Neurosurg Psychiatry 2001 71:149-154Giovanni HenryPas encore d'évaluation
- Defining Physiology: Principles, Themes, Concepts.: Hwee Ming Cheng Kin Kheong Mah Kumar SeluakumaranDocument104 pagesDefining Physiology: Principles, Themes, Concepts.: Hwee Ming Cheng Kin Kheong Mah Kumar SeluakumaranGiovanni HenryPas encore d'évaluation
- Sept 2020 MRCS RecallsDocument46 pagesSept 2020 MRCS RecallsGiovanni Henry75% (4)
- Endothelium I: Atherogenesis: Maintenance of Vascular HomeostasisDocument5 pagesEndothelium I: Atherogenesis: Maintenance of Vascular HomeostasisGiovanni HenryPas encore d'évaluation
- September 2020 Recalls Scorpio and Al Beruni 243 QuestionsDocument9 pagesSeptember 2020 Recalls Scorpio and Al Beruni 243 QuestionsGiovanni HenryPas encore d'évaluation
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- The Physiology of Human DefecationDocument21 pagesThe Physiology of Human Defecationyohanna yohannaPas encore d'évaluation
- April 2018 IMRCS A Exam ReviewDocument12 pagesApril 2018 IMRCS A Exam Reviewmobz00Pas encore d'évaluation
- Medical EMQs and Clinical ScenariosDocument18 pagesMedical EMQs and Clinical ScenariosMehdi Hasan MazumderPas encore d'évaluation
- Gen Surg 1996 2009Document26 pagesGen Surg 1996 2009LijoeliyasPas encore d'évaluation
- Transplantation: Leo-Paul Powell DM Tutorial Series March 30, 2021Document45 pagesTransplantation: Leo-Paul Powell DM Tutorial Series March 30, 2021Giovanni HenryPas encore d'évaluation
- Surgical AnatomyDocument4 pagesSurgical AnatomyGiovanni HenryPas encore d'évaluation
- April 2018 Recalls - Reda: Embolectomy??)Document5 pagesApril 2018 Recalls - Reda: Embolectomy??)Giovanni HenryPas encore d'évaluation
- DNB Gen Surgery Old Question Papers 1Document28 pagesDNB Gen Surgery Old Question Papers 1sidorai100% (1)
- Surgery Questions EssayDocument11 pagesSurgery Questions Essaymimycutey100% (3)
- General Surgery June 2010: Paper IDocument2 pagesGeneral Surgery June 2010: Paper IGiovanni HenryPas encore d'évaluation
- Colon & Rectum Questions Aug 2008Document61 pagesColon & Rectum Questions Aug 2008Dr.mesho Bin MansourPas encore d'évaluation
- DNB Gen Surgery Old Question Papers 1Document28 pagesDNB Gen Surgery Old Question Papers 1sidorai100% (1)
- Frcs Viva TOPICSDocument4 pagesFrcs Viva TOPICSGiovanni HenryPas encore d'évaluation
- EVAR vs. Open Repair - EvidenceDocument5 pagesEVAR vs. Open Repair - EvidenceGiovanni HenryPas encore d'évaluation
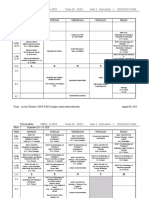
- Class of 2023 Year 1 Sem 1 Final Aug 30Document16 pagesClass of 2023 Year 1 Sem 1 Final Aug 30Giovanni HenryPas encore d'évaluation
- Facts and Figures: Sleep ApneaDocument2 pagesFacts and Figures: Sleep ApneaNazir AhmadPas encore d'évaluation
- Answered Step-By-Step: Answer & Explanation Related Questions Related CoursesDocument6 pagesAnswered Step-By-Step: Answer & Explanation Related Questions Related CoursesEddyOmburahPas encore d'évaluation
- CMS Psychiatry 1 FormDocument41 pagesCMS Psychiatry 1 FormDuriye Damla Sevgi100% (6)
- ARDS Concept Map - BunayogDocument2 pagesARDS Concept Map - BunayogJacela Annsyle BunayogPas encore d'évaluation
- A Community-Based Mothers and Infants CenterDocument10 pagesA Community-Based Mothers and Infants CenterRazonable Morales RommelPas encore d'évaluation
- Pil 2200016 28112017185241 636474919780156250Document4 pagesPil 2200016 28112017185241 636474919780156250HjkjPas encore d'évaluation
- Japanese Encephalitis Causes, Symptoms, TreatmentDocument9 pagesJapanese Encephalitis Causes, Symptoms, TreatmentAhmed Mawardi0% (1)
- 2014 Convocation in Colorado Springs Evening With The FAAO's Program-6Document3 pages2014 Convocation in Colorado Springs Evening With The FAAO's Program-6Dr-Syed Hammad Hussain-GilaniPas encore d'évaluation
- Pott DiseaseDocument36 pagesPott DiseaseGiovanna Algu100% (1)
- HIV Transmission, Pathophysiology, Clinical Manifestations and TreatmentDocument4 pagesHIV Transmission, Pathophysiology, Clinical Manifestations and TreatmentBatch V Med 2 SY 21-22Pas encore d'évaluation
- Centor ScoreDocument8 pagesCentor ScoreLoo DonPas encore d'évaluation
- Spinal Tumor StrongDocument45 pagesSpinal Tumor StrongbettyPas encore d'évaluation
- HonkDocument22 pagesHonkSitta Grewo LiandarPas encore d'évaluation
- Pharmacotherapy of heart failureDocument79 pagesPharmacotherapy of heart failureAbera JamboPas encore d'évaluation
- DUTY SDH + CKDDocument6 pagesDUTY SDH + CKDadelia putri wirandaniPas encore d'évaluation
- Rare RemediesDocument26 pagesRare RemediesMuhammad Ata Ul MustafaPas encore d'évaluation
- LESSON PLAN 6 MALARIA IN PREGNANCYjjDocument13 pagesLESSON PLAN 6 MALARIA IN PREGNANCYjjjrkedridgemwanakalandoPas encore d'évaluation
- DMSF College of Nursing Anatomy and Physiology MDTERMS QUIZ 1Document2 pagesDMSF College of Nursing Anatomy and Physiology MDTERMS QUIZ 1Trisha TamsiPas encore d'évaluation
- 1 - Series 2022Document9 pages1 - Series 2022Vijay U100% (1)
- Oa Case ReportDocument26 pagesOa Case Reportaliffikri52100% (1)
- Cerebral Palsy Causes and Classification GuideDocument40 pagesCerebral Palsy Causes and Classification Guiderenuka aurangabadkerPas encore d'évaluation
- Assessment of Renal and Urinary Tract FunctionDocument40 pagesAssessment of Renal and Urinary Tract FunctionBjorn Francisco100% (1)
- Sunil Prabhudev SonpawaleDocument3 pagesSunil Prabhudev SonpawaleSunil SonpawalePas encore d'évaluation
- Management For PancreatolithiasisDocument13 pagesManagement For PancreatolithiasisAhmad Fakhrozi HelmiPas encore d'évaluation
- Differential Diagnosis of Cheilitis - How To ClassDocument11 pagesDifferential Diagnosis of Cheilitis - How To ClassRonaldo PutraPas encore d'évaluation
- GDM Nice GuidelinesDocument56 pagesGDM Nice GuidelinesArfa NageenPas encore d'évaluation
- Not PrecedentialDocument20 pagesNot PrecedentialScribd Government DocsPas encore d'évaluation
- Pre and Post-Operative Care of Patient For Mastectomy: Prepared By: Gianne T. Gregorio RNDocument13 pagesPre and Post-Operative Care of Patient For Mastectomy: Prepared By: Gianne T. Gregorio RNmalathiPas encore d'évaluation
- Tugas Bahasa Inggris "Roleplay Ambulation": OlehDocument3 pagesTugas Bahasa Inggris "Roleplay Ambulation": Olehnono NonoPas encore d'évaluation
- Patient Details Patient ID: Temp: BP: Weight: Height: Consultation ID: Date: Mode of Consult: Follow UpDocument1 pagePatient Details Patient ID: Temp: BP: Weight: Height: Consultation ID: Date: Mode of Consult: Follow UpSabari PramanikPas encore d'évaluation