Vous aimerez peut-être aussi
- Valvular Heart DiseaseDocument85 pagesValvular Heart DiseaseWilliam Lie100% (2)
- ICE8112 Hazard of The Harad Wood (OCR) (T)Document34 pagesICE8112 Hazard of The Harad Wood (OCR) (T)Percy PersimmonPas encore d'évaluation
- Clinical ChemistryDocument24 pagesClinical ChemistryQueency Dangilan100% (1)
- Congenital Heart Disease (CHD) : Kussia Ayano (MD)Document54 pagesCongenital Heart Disease (CHD) : Kussia Ayano (MD)Yemata HailuPas encore d'évaluation
- Right Ventricular Myocardial InfarctionDocument43 pagesRight Ventricular Myocardial Infarctionrudresh m g0% (2)
- Aortic RegurgitationDocument12 pagesAortic RegurgitationSanjeet SahPas encore d'évaluation
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtD'EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtÉvaluation : 5 sur 5 étoiles5/5 (1)
- Congenital Heart DiseaseDocument6 pagesCongenital Heart DiseaseSamah KhanPas encore d'évaluation
- Aortic StenosisDocument37 pagesAortic Stenosissarguss14Pas encore d'évaluation
- X-Ray CVSDocument67 pagesX-Ray CVSmdjohariPas encore d'évaluation
- Neonatal Heart DiseaseDocument8 pagesNeonatal Heart DiseaseDelphy VarghesePas encore d'évaluation
- Rheumatic Heart DiseaseDocument47 pagesRheumatic Heart DiseaseGideon K. MutaiPas encore d'évaluation
- Prolapsed Intervertebral Disc: By: Diksha Solanki Bot 4 YearDocument37 pagesProlapsed Intervertebral Disc: By: Diksha Solanki Bot 4 YearISIC IRS100% (1)
- Counselling Plab2Aspired19Document137 pagesCounselling Plab2Aspired19osamaePas encore d'évaluation
- Meet The Profesor 2021Document398 pagesMeet The Profesor 2021Raúl AssadPas encore d'évaluation
- Clopidogrel Bisulfate (PLOGREL)Document2 pagesClopidogrel Bisulfate (PLOGREL)Kristine Young0% (1)
- Big Data and GenomicsDocument54 pagesBig Data and GenomicsNational Press FoundationPas encore d'évaluation
- MRCP Revision NotesDocument41 pagesMRCP Revision NotesMudassar Waseem100% (1)
- Renal MCQ 4Document10 pagesRenal MCQ 4AzizPas encore d'évaluation
- Valvular Heart DiseaseDocument73 pagesValvular Heart Diseaseindia2puppy100% (4)
- Cardiac Tamponade and ManagementDocument42 pagesCardiac Tamponade and Managementأم حمدPas encore d'évaluation
- Kuliah MITRAL STENOSISDocument19 pagesKuliah MITRAL STENOSISekaseptiani312Pas encore d'évaluation
- Valvular Heart Disease: Departemen Kardiologi Dan Kedokteran Vaskular FK UsuDocument38 pagesValvular Heart Disease: Departemen Kardiologi Dan Kedokteran Vaskular FK UsuDumora FatmaPas encore d'évaluation
- K7 - Penyakit Jantung Katub-ANNDocument38 pagesK7 - Penyakit Jantung Katub-ANNXeniel AlastairPas encore d'évaluation
- Valvular Heart Disease: Bekele T. (MD)Document47 pagesValvular Heart Disease: Bekele T. (MD)alehegn beletePas encore d'évaluation
- Mitral Regurgitation: MedicineDocument7 pagesMitral Regurgitation: Medicineapi-3829364Pas encore d'évaluation
- CVS1 - K8 - Valvular Heart DiseaseDocument79 pagesCVS1 - K8 - Valvular Heart DiseaseDumora FatmaPas encore d'évaluation
- (K7) Valvular Heart DiseaseDocument79 pages(K7) Valvular Heart DiseaseXeniel AlastairPas encore d'évaluation
- Pathophysiology of Pericardial DiseaseDocument36 pagesPathophysiology of Pericardial DiseaseivaniPas encore d'évaluation
- Congenital Heart Disease-2Document57 pagesCongenital Heart Disease-2Deepika LamichhanePas encore d'évaluation
- Kuliah MITRAL STENOSISDocument19 pagesKuliah MITRAL STENOSISAdi TrisnoPas encore d'évaluation
- Rheumatic Heart DiseaseDocument30 pagesRheumatic Heart DiseaseDhiraj PantPas encore d'évaluation
- Valvular Heart DiseaseDocument5 pagesValvular Heart DiseaseElyas MehdarPas encore d'évaluation
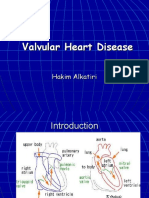
- Valvular Heart Disease: Hakim AlkatiriDocument84 pagesValvular Heart Disease: Hakim AlkatiriFPas encore d'évaluation
- 3 CRHD CMP and CHDDocument73 pages3 CRHD CMP and CHDDammaqsaa W BiyyanaaPas encore d'évaluation
- Pulmonic Valve DiseaseDocument22 pagesPulmonic Valve Diseasesarguss14Pas encore d'évaluation
- Management of Rheumatic Heart Disease: Quick Reference Guide For Health ProfessionalsDocument4 pagesManagement of Rheumatic Heart Disease: Quick Reference Guide For Health ProfessionalsgireeshsachinPas encore d'évaluation
- Penyakit Katup Jantung: Dr. Tjatur Winarsanto SPPD Rs CiremaiDocument59 pagesPenyakit Katup Jantung: Dr. Tjatur Winarsanto SPPD Rs CiremaianisamayaPas encore d'évaluation
- Valvular UpdateDocument44 pagesValvular UpdateUlmi FadillahPas encore d'évaluation
- Rheumatic Heart Disease2Document61 pagesRheumatic Heart Disease2Puji Yunisyah RahayuPas encore d'évaluation
- Mitral Stenosis: Dr. Mohammed Asrafur Rahman MBBS, Bcs (H), MD Resident (Internal Medicine) (P-A) Chattogram Medical CollegeDocument16 pagesMitral Stenosis: Dr. Mohammed Asrafur Rahman MBBS, Bcs (H), MD Resident (Internal Medicine) (P-A) Chattogram Medical CollegeAsrafur RahmanPas encore d'évaluation
- KP 2.3.1.6Document42 pagesKP 2.3.1.6Taufiqurrahman HabibPas encore d'évaluation
- Penyakit Katup Jantung-Kuliah DR ErlinaDocument70 pagesPenyakit Katup Jantung-Kuliah DR ErlinaAdhiatma DotPas encore d'évaluation
- Rheumatic Heart DiseaseDocument35 pagesRheumatic Heart DiseaseSAYMABANUPas encore d'évaluation
- 28 Valvular Heart Disease DR - YusraDocument46 pages28 Valvular Heart Disease DR - YusraSurya ArhPas encore d'évaluation
- Pathophys VHD-Final (Budi S. Pikir)Document155 pagesPathophys VHD-Final (Budi S. Pikir)Muhammad DaviqPas encore d'évaluation
- Cvs-k7-Valvular Heart Disease Nora2010Document52 pagesCvs-k7-Valvular Heart Disease Nora2010shiloinPas encore d'évaluation
- CVS 3-3 PDFDocument24 pagesCVS 3-3 PDFafaq alismailiPas encore d'évaluation
- 4 Valvular Heart Disease#36f7Document40 pages4 Valvular Heart Disease#36f7Natasha LiberisPas encore d'évaluation
- Management of Cyanotic Child BivinDocument48 pagesManagement of Cyanotic Child BivinChippy BivinPas encore d'évaluation
- Medicine: Aquired Valvular Heart DiseaseDocument3 pagesMedicine: Aquired Valvular Heart Diseaseapi-3829364Pas encore d'évaluation
- Valvular Heart DiseaseDocument34 pagesValvular Heart DiseaseRebecca FeltonPas encore d'évaluation
- Valvular Heart Disease: Dr. Nigussie BerihunDocument43 pagesValvular Heart Disease: Dr. Nigussie Berihunsisay tigabuPas encore d'évaluation
- 10 1016@j CCL 2020 04 008Document12 pages10 1016@j CCL 2020 04 008Linda Silvana SariPas encore d'évaluation
- Dr. Musnidarti, SPJP, FihaDocument72 pagesDr. Musnidarti, SPJP, FihasovianPas encore d'évaluation
- Curs 4 Urgente in Cardiologie Anul VI Seriile A B C DDocument35 pagesCurs 4 Urgente in Cardiologie Anul VI Seriile A B C DBoţu AlexandruPas encore d'évaluation
- VHD Inter FinalDocument84 pagesVHD Inter Finalfitrah fajrianiPas encore d'évaluation
- Aortic Regurgitation CaseDocument38 pagesAortic Regurgitation CaseIka MagfirahPas encore d'évaluation
- CCHDDocument69 pagesCCHDchebetnaomi945Pas encore d'évaluation
- Valvular Heart Disease 2Document46 pagesValvular Heart Disease 2Topea BogdanPas encore d'évaluation
- Right Ventricular Failure: Pathophysiology, Diagnosis and TreatmentDocument16 pagesRight Ventricular Failure: Pathophysiology, Diagnosis and TreatmentRizky Regia TriseynesyaPas encore d'évaluation
- Valvular Heart DiseaseDocument27 pagesValvular Heart DiseaseCharlz ZipaganPas encore d'évaluation
- Pemicu 6 Eko Blok KGDDocument128 pagesPemicu 6 Eko Blok KGDEko SiswantoPas encore d'évaluation
- Fever and Murmurs and Infective EndocarditisDocument13 pagesFever and Murmurs and Infective EndocarditishalesPas encore d'évaluation
- Nursing Acn-IiDocument80 pagesNursing Acn-IiMunawar100% (6)
- Cardiac Care and COVID-19: Perspectives in Medical PracticeD'EverandCardiac Care and COVID-19: Perspectives in Medical PracticePas encore d'évaluation
- Intrinsic Conducting System - CVS-K2 UmsuDocument44 pagesIntrinsic Conducting System - CVS-K2 Umsudwi ariskaPas encore d'évaluation
- Obat Antiaritmia: Departemen Farmakologi Dan Terapeutik Fakultas Kedokteran Universitas Muhammadiyah Sumatera UtaraDocument20 pagesObat Antiaritmia: Departemen Farmakologi Dan Terapeutik Fakultas Kedokteran Universitas Muhammadiyah Sumatera Utaradwi ariskaPas encore d'évaluation
- Cardio Vas Cul ErDocument68 pagesCardio Vas Cul Erdwi ariskaPas encore d'évaluation
- Laporan Praktikum Farmakologi Obat Mata: Fakultas Kedokteran UmsuDocument2 pagesLaporan Praktikum Farmakologi Obat Mata: Fakultas Kedokteran Umsudwi ariskaPas encore d'évaluation
- Daftar Pustaka: Operasional (SPO) Neurologi.2006Document1 pageDaftar Pustaka: Operasional (SPO) Neurologi.2006dwi ariskaPas encore d'évaluation
- Proposal: PK Imm Fakultas Kedokteran UmsuDocument2 pagesProposal: PK Imm Fakultas Kedokteran Umsudwi ariskaPas encore d'évaluation
- Biochemistry 090819Document33 pagesBiochemistry 090819Abhishek PawarPas encore d'évaluation
- Reagen Dan Instrumen Pendukung Untuk Laboratorium Pengujian COVID-19Document14 pagesReagen Dan Instrumen Pendukung Untuk Laboratorium Pengujian COVID-19Mike SihombingPas encore d'évaluation
- IndianJPsychiatry618254-624277 172027Document16 pagesIndianJPsychiatry618254-624277 172027Fatma BakrPas encore d'évaluation
- Failure of Endoscopic Spine SurgeryDocument6 pagesFailure of Endoscopic Spine SurgeryKaustubh KeskarPas encore d'évaluation
- Cardiac Rehabilitation.Document60 pagesCardiac Rehabilitation.Salman KhanPas encore d'évaluation
- Treatment Guidelines For Hyponatremia Stay The.180Document22 pagesTreatment Guidelines For Hyponatremia Stay The.180Carolyn CamposPas encore d'évaluation
- Discussion Question 1Document3 pagesDiscussion Question 1Brian RelsonPas encore d'évaluation
- HomeostasisDocument2 pagesHomeostasisAnn Calindo EstafiaPas encore d'évaluation
- 4 Drug Development ProcessDocument9 pages4 Drug Development ProcessMicah MontePas encore d'évaluation
- Cardiovascular SystemDocument9 pagesCardiovascular SystemMayim LouisePas encore d'évaluation
- Medical TranslationDocument13 pagesMedical TranslationИванка СакареваPas encore d'évaluation
- Pengetahuan Mengenai Faktor Risiko Dan Perilaku Pasien Sindrom Koroner Akut Jeki RefialdinataDocument10 pagesPengetahuan Mengenai Faktor Risiko Dan Perilaku Pasien Sindrom Koroner Akut Jeki RefialdinataFATIMAH WANDAPas encore d'évaluation
- 2022 09 10NewScientistDocument60 pages2022 09 10NewScientistAyala AbishevaPas encore d'évaluation
- Bioinformatics DatabaseDocument50 pagesBioinformatics DatabasedhanushumakanthaPas encore d'évaluation
- Aedes Egypti ADocument10 pagesAedes Egypti AOswin YohsaPas encore d'évaluation
- LDN Information PackDocument17 pagesLDN Information PackkindheartedPas encore d'évaluation
- Medical Rehabilitation in Compression FractureDocument32 pagesMedical Rehabilitation in Compression FracturegloriaPas encore d'évaluation
- Spinal StenosisDocument14 pagesSpinal StenosisHONGJYPas encore d'évaluation
- Medicare PAP Documentation Requirements - Supplier Self-Audit ChecklistDocument2 pagesMedicare PAP Documentation Requirements - Supplier Self-Audit CheckliststevierayoPas encore d'évaluation
- MED TECH Clinical ChemistryDocument3 pagesMED TECH Clinical ChemistryJan Martin Mogueis JustoPas encore d'évaluation
- Rural Awareness Work Experience Programme Manual: B.Sc. (Hons.) HorticultureDocument88 pagesRural Awareness Work Experience Programme Manual: B.Sc. (Hons.) HorticulturePotsangbam Dhanabir SinghPas encore d'évaluation
- Rds CaseDocument42 pagesRds Casegebby puspitaPas encore d'évaluation