Vous aimerez peut-être aussi
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Fluid Manajemen in Pre EclampsiaDocument39 pagesFluid Manajemen in Pre EclampsiaJinan Fairuz Anindika RPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- P 852Document8 pagesP 852Jinan Fairuz Anindika RPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Ondansetron GRDocument8 pagesOndansetron GRJinan Fairuz Anindika RPas encore d'évaluation
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Fluid Manajemen in Pre EclampsiaDocument39 pagesFluid Manajemen in Pre EclampsiaJinan Fairuz Anindika RPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Heart FailureDocument23 pagesHeart FailureJinan Fairuz Anindika RPas encore d'évaluation
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Cor PulmonaleDocument10 pagesCor PulmonaleJinan Fairuz Anindika RPas encore d'évaluation
- Exploring The Factors Affecting Motorway Accident Severity in EnglandDocument9 pagesExploring The Factors Affecting Motorway Accident Severity in EnglandJinan Fairuz Anindika RPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Clinical DiagnosisDocument2 pagesClinical DiagnosisJinan Fairuz Anindika RPas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Teknik AseptikDocument18 pagesTeknik AseptikAisya FikritamaPas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Clinical DiagnosisDocument2 pagesClinical DiagnosisJinan Fairuz Anindika RPas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Ja2014 983635Document7 pagesJa2014 983635Jinan Fairuz Anindika RPas encore d'évaluation
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A1 Template V5Document1 pageA1 Template V5Jinan Fairuz Anindika RPas encore d'évaluation
- Minggu: P. Wanita P. Pria Infeksi/Bedah R.Tindakan/Alergi Kosmetik Kamis Jum'at Sabtu Senin Selasa Rabu Kamis Jum'atDocument3 pagesMinggu: P. Wanita P. Pria Infeksi/Bedah R.Tindakan/Alergi Kosmetik Kamis Jum'at Sabtu Senin Selasa Rabu Kamis Jum'atJinan Fairuz Anindika RPas encore d'évaluation
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Warna Warni Jurnal Dari Prof OsDocument9 pagesWarna Warni Jurnal Dari Prof OsJinan Fairuz Anindika RPas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Daftar PustakaDocument5 pagesDaftar PustakaJinan Fairuz Anindika RPas encore d'évaluation
- Format Rekap Data InputDocument8 pagesFormat Rekap Data InputJinan Fairuz Anindika RPas encore d'évaluation
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Print BINGODocument25 pagesPrint BINGOJinan Fairuz Anindika RPas encore d'évaluation
- ReadmeDocument1 pageReadmeJinan Fairuz Anindika RPas encore d'évaluation
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Evaluasi NeurologikDocument3 pagesEvaluasi NeurologikJinan Fairuz Anindika RPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Curriculum VitaeDocument12 pagesCurriculum VitaeHannah AlmacenPas encore d'évaluation
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- DR Lie Khie Chen - Management of MDR Infection in Sepsis Jade 2016Document33 pagesDR Lie Khie Chen - Management of MDR Infection in Sepsis Jade 2016Astria PermanaPas encore d'évaluation
- Burns: Hadi Munib Oral and Maxillofacial SurgeryDocument79 pagesBurns: Hadi Munib Oral and Maxillofacial SurgeryAli ahmedPas encore d'évaluation
- Seven Senses Chakra GuideDocument11 pagesSeven Senses Chakra GuidemhliuPas encore d'évaluation
- Croup: Assessment and ManagementDocument3 pagesCroup: Assessment and Managementsandra magdalenaPas encore d'évaluation
- Narrative Report On Second Sem SyllabusDocument92 pagesNarrative Report On Second Sem SyllabusChristine Joy MolinaPas encore d'évaluation
- Bones and Joints Quiz Questions - Footprints-Science GCSE Science Animations and QuizzesDocument1 pageBones and Joints Quiz Questions - Footprints-Science GCSE Science Animations and Quizzescpcp6n7tc5Pas encore d'évaluation
- Life Is A Continous Process of AdjustmentDocument78 pagesLife Is A Continous Process of AdjustmentGulmoharPas encore d'évaluation
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (120)
- Genetics Notes - Other Patterns of Inheritance & PedigreesDocument4 pagesGenetics Notes - Other Patterns of Inheritance & PedigreesJoseph Dav6657Pas encore d'évaluation
- Lumber Mold - WPPA - Mold-Housing-Wood-Tg2Document12 pagesLumber Mold - WPPA - Mold-Housing-Wood-Tg2Jeff HPas encore d'évaluation
- The Theory of Schussler's Biochemic MethodDocument11 pagesThe Theory of Schussler's Biochemic MethodpankajgoelpnpPas encore d'évaluation
- Shock Comparison ChartDocument2 pagesShock Comparison Chartlinnaete88% (8)
- Best Practice Guidelines - Wound Management Diabetic Foot UlcersDocument27 pagesBest Practice Guidelines - Wound Management Diabetic Foot UlcersAndrada Catrinoiu100% (1)
- Hydrogen Hydroxide: Acid-Base Balance Overview of Acids and Bases DescriptionDocument15 pagesHydrogen Hydroxide: Acid-Base Balance Overview of Acids and Bases DescriptionElisha WorworPas encore d'évaluation
- Chapter 13 - Diseases of White Blood Cells, Lymph Nodes, Spleen, and ThymusDocument10 pagesChapter 13 - Diseases of White Blood Cells, Lymph Nodes, Spleen, and ThymusAgnieszka WisniewskaPas encore d'évaluation
- Godbout, J. P., & Glaser, R. (2006) - Stress-Induced Immune Dysregulation. Implications For Wound Healing, Infectious Disease and CancerDocument7 pagesGodbout, J. P., & Glaser, R. (2006) - Stress-Induced Immune Dysregulation. Implications For Wound Healing, Infectious Disease and CancerFranco Paolo Maray-GhigliottoPas encore d'évaluation
- Mathematical Modeling of COVID-19 Spreading With Asymptomatic Infected and Interacting PeoplesDocument23 pagesMathematical Modeling of COVID-19 Spreading With Asymptomatic Infected and Interacting PeoplesYjhvhgjvPas encore d'évaluation
- San Jiao Chap 12Document3 pagesSan Jiao Chap 12Bolt VoPas encore d'évaluation
- Clinical Diagnostic Criteria For Dementia AssociatDocument20 pagesClinical Diagnostic Criteria For Dementia AssociatAnderson Cassol DozzaPas encore d'évaluation
- Factors Impacting Food Workers and Managers Safe Food Preparation PracticesDocument28 pagesFactors Impacting Food Workers and Managers Safe Food Preparation PracticesSteffi Grace100% (1)
- Antibiotic Resistance and Evolution Case Study GR 11Document7 pagesAntibiotic Resistance and Evolution Case Study GR 11Petro BricalliPas encore d'évaluation
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Management of Trauma PatientsDocument4 pagesManagement of Trauma PatientsAhmed ShehataPas encore d'évaluation
- OpenTexas Checklist Overnight Youth Camp: FamiliesDocument3 pagesOpenTexas Checklist Overnight Youth Camp: FamiliesRebecca Salinas100% (1)
- CBC Arikod HoimaDocument37 pagesCBC Arikod Hoimadaniel arikodPas encore d'évaluation
- Urinary System and Its PathologiesDocument23 pagesUrinary System and Its Pathologiesngachangong victorinePas encore d'évaluation
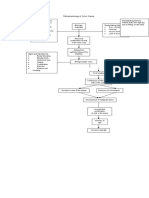
- Pathophysiology of Colon Cancer Predisposing Factors: Etiology: Precipitating Factors: Precipitating FactorsDocument1 pagePathophysiology of Colon Cancer Predisposing Factors: Etiology: Precipitating Factors: Precipitating FactorstatiPas encore d'évaluation
- Bleeding DisorderDocument3 pagesBleeding DisorderyanzwinerPas encore d'évaluation
- Cholecystitis: By: Myla Rojas. BalandraDocument5 pagesCholecystitis: By: Myla Rojas. BalandraMyla Rojas BalandraPas encore d'évaluation
- History of Microbiology 16th CENTURYDocument3 pagesHistory of Microbiology 16th CENTURYMeangel QuillaoPas encore d'évaluation
- Pulses: Shu Chi HuanDocument1 pagePulses: Shu Chi HuanRicardo TeixeiraPas encore d'évaluation
- Uncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicD'EverandUncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicPas encore d'évaluation
- Deaths of Despair and the Future of CapitalismD'EverandDeaths of Despair and the Future of CapitalismÉvaluation : 4.5 sur 5 étoiles4.5/5 (30)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisD'EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisÉvaluation : 4 sur 5 étoiles4/5 (9)