Vous aimerez peut-être aussi
- Posterior Polar Cataract Management: My Approach: 2022, #1D'EverandPosterior Polar Cataract Management: My Approach: 2022, #1Pas encore d'évaluation
- Button Battery Ingestion Birmingham Childrens Hospital 2013Document1 pageButton Battery Ingestion Birmingham Childrens Hospital 2013rashidPas encore d'évaluation
- 105 Instillations Intra-Vesicales de BCGDocument7 pages105 Instillations Intra-Vesicales de BCGAndreea GrigaPas encore d'évaluation
- IUD Complications: Management Strategies: Learning ObjectivesDocument9 pagesIUD Complications: Management Strategies: Learning ObjectivesIndah Putri permatasariPas encore d'évaluation
- 4.MEDICAL AND SURGICAL MANAGEMENT (Table 3)Document5 pages4.MEDICAL AND SURGICAL MANAGEMENT (Table 3)SONY MANDAPPas encore d'évaluation
- NCP Impaired Skin IntegrityDocument2 pagesNCP Impaired Skin IntegrityMarc Johnuel HumangitPas encore d'évaluation
- QPCM, Specimen Collection Guide, Mount Sinai, GovDocument74 pagesQPCM, Specimen Collection Guide, Mount Sinai, GovFilipus HendiantoPas encore d'évaluation
- Oxytetracycline - Casimero (Group41)Document2 pagesOxytetracycline - Casimero (Group41)Hannah Angela CasimeroPas encore d'évaluation
- DRUG STUDY Irinotecan hydrochloride study at Brokenshire CollegeDocument3 pagesDRUG STUDY Irinotecan hydrochloride study at Brokenshire CollegeJai GoPas encore d'évaluation
- Ad EmergencycardDocument2 pagesAd EmergencycardAlysse GavlikPas encore d'évaluation
- Drug StudyDocument13 pagesDrug StudygemzkeePas encore d'évaluation
- Nursing Care Plan for Baby Jason with Cleft Lip and PalateDocument3 pagesNursing Care Plan for Baby Jason with Cleft Lip and PalatePatricia Ellyne DizonPas encore d'évaluation
- Anchorage of Partial Avulsion of The Heel Pad With Use of Multiple Kirschner WiresDocument4 pagesAnchorage of Partial Avulsion of The Heel Pad With Use of Multiple Kirschner WiresPrabhjeet singhPas encore d'évaluation
- Drug Study PDFDocument7 pagesDrug Study PDFMarissa AsimPas encore d'évaluation
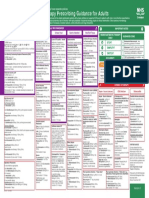
- Empirical Antimicrobial Therapy Prescribing Guidance For AdultsDocument1 pageEmpirical Antimicrobial Therapy Prescribing Guidance For AdultsPsychology TodayPas encore d'évaluation
- SUMAOANG - Maalox Drug StudyDocument4 pagesSUMAOANG - Maalox Drug StudyMina SumaoangPas encore d'évaluation
- Gehc Care Card Tee Probe Care CardDocument2 pagesGehc Care Card Tee Probe Care CardIqra ChuhanPas encore d'évaluation
- MRSA Contact Precautions Removal AlgorithmDocument1 pageMRSA Contact Precautions Removal Algorithmbayu bayuPas encore d'évaluation
- Complicated Community Acquired Pneumonia Clinical PathwayDocument14 pagesComplicated Community Acquired Pneumonia Clinical PathwayFaisalMuhamadPas encore d'évaluation
- Chemotherapeutic AgentDocument16 pagesChemotherapeutic AgentAngelica PabelloPas encore d'évaluation
- Ultimate TENS User Manual Prescribing InfoDocument12 pagesUltimate TENS User Manual Prescribing InfoAndreas Arie WidiadiaksaPas encore d'évaluation
- Albothyl Solution Successfully Cured A Case With.34Document2 pagesAlbothyl Solution Successfully Cured A Case With.34Kikin RizkynnisaPas encore d'évaluation
- GROUP1 Drug Therapeutic RecordDocument6 pagesGROUP1 Drug Therapeutic RecordYori Nicole Martine CuyosPas encore d'évaluation
- ติว NL2 ปี 5 2022 outlineDocument49 pagesติว NL2 ปี 5 2022 outlineSugus PichayaPas encore d'évaluation
- Name of Drug Mechanism of Action Contraindication Side Effects Adverse Effects Nursing ResponsibilitiesDocument2 pagesName of Drug Mechanism of Action Contraindication Side Effects Adverse Effects Nursing ResponsibilitiesMichelle Dona MirallesPas encore d'évaluation
- Syndromic ManagemtDocument4 pagesSyndromic ManagemtKain ValkyriePas encore d'évaluation
- Ceftazidime (Zeptrigen)Document4 pagesCeftazidime (Zeptrigen)105990Pas encore d'évaluation
- Drugs Drugs DtugsDocument11 pagesDrugs Drugs Dtugs105990Pas encore d'évaluation
- Case 1Document9 pagesCase 1Joselyn M. LachicaPas encore d'évaluation
- JAMBALOS JERALDEEN BSN 4 2 DRUG STUDY FormatDocument3 pagesJAMBALOS JERALDEEN BSN 4 2 DRUG STUDY FormatJeraldeen JambalosPas encore d'évaluation
- Pil 76Document4 pagesPil 76IyaadanPas encore d'évaluation
- Endoscopic Surgery of The OrbitDocument5 pagesEndoscopic Surgery of The OrbitTugce IncePas encore d'évaluation
- NCP Impaired Skin IntegrityDocument2 pagesNCP Impaired Skin Integritysnay axiePas encore d'évaluation
- 6 Drug StudyDocument12 pages6 Drug StudyBabylayne PangcatanPas encore d'évaluation
- Drug Study - CefuroximeDocument2 pagesDrug Study - CefuroximeReal TetisoraPas encore d'évaluation
- Don Mariano Marcos Memorial State University Nursing CaseDocument9 pagesDon Mariano Marcos Memorial State University Nursing CaseJoselyn M. LachicaPas encore d'évaluation
- Module 3 - Case 1Document9 pagesModule 3 - Case 1Joselyn M. LachicaPas encore d'évaluation
- DRUG+STUDY NaprexDocument2 pagesDRUG+STUDY NaprexJoevence Gazo CuaresmaPas encore d'évaluation
- TELAVANCIN DRUG MECHANISM AND NURSING RESPONSIBILITIESDocument2 pagesTELAVANCIN DRUG MECHANISM AND NURSING RESPONSIBILITIESEmilie CajaPas encore d'évaluation
- HealthDocument1 pageHealthUp ApPas encore d'évaluation
- Ketorolac DRUG STUDYDocument3 pagesKetorolac DRUG STUDYA.Pas encore d'évaluation
- DS - Mod9Document2 pagesDS - Mod9designericlelynsoronioPas encore d'évaluation
- Intestinal ParasitesDocument1 pageIntestinal ParasitesSabir YeddiPas encore d'évaluation
- Diarrhea Decision TreeDocument1 pageDiarrhea Decision TreeMatthew BrandPas encore d'évaluation
- NCP and Drug Study Form APDocument6 pagesNCP and Drug Study Form APRed EslaoPas encore d'évaluation
- Paediatric Clinical Practice Guideline Ingestion of Foreign Bodies (FB)Document4 pagesPaediatric Clinical Practice Guideline Ingestion of Foreign Bodies (FB)AdaMariaBalanPas encore d'évaluation
- 3) Enteral AdministrationDocument11 pages3) Enteral AdministrationdullnesangelPas encore d'évaluation
- NCM 112 LecDocument8 pagesNCM 112 LecGEOMHAI CATBAGANPas encore d'évaluation
- Small Bowel Obstruction System - DisorderDocument1 pageSmall Bowel Obstruction System - DisorderMarina Wasem Netzlaff0% (1)
- Dabe Drug StudyDocument3 pagesDabe Drug StudyMary Joy Anne LucasPas encore d'évaluation
- PB3 NP1Document10 pagesPB3 NP1Angelica Charisse BuliganPas encore d'évaluation
- Drugs Study Post VaricocoelectomyDocument2 pagesDrugs Study Post VaricocoelectomyIris CabertePas encore d'évaluation
- Intralesional Ethanol For An Unresectable Epithelial Inclusion CystDocument2 pagesIntralesional Ethanol For An Unresectable Epithelial Inclusion CystJave GajellomaPas encore d'évaluation
- Paediatric Guidelines Foreign Body Ingestion 2018 1Document5 pagesPaediatric Guidelines Foreign Body Ingestion 2018 1Bîcă OvidiuPas encore d'évaluation
- Ocular Emergencies GuideDocument6 pagesOcular Emergencies GuidePatricia ManaliliPas encore d'évaluation
- Catheter-Associated Urinary Tract Infection (CAUTI) : Prevention Diagnosis and ManagementDocument6 pagesCatheter-Associated Urinary Tract Infection (CAUTI) : Prevention Diagnosis and ManagementTamil SelvaPas encore d'évaluation
- 11december2020 20201211 Clinical Management Guidelines For COVID-19 Infection 1204Document14 pages11december2020 20201211 Clinical Management Guidelines For COVID-19 Infection 1204Jawariya ZiaPas encore d'évaluation
- Case Scenario Typhoid FeverDocument5 pagesCase Scenario Typhoid FeverMae Arra Lecobu-anPas encore d'évaluation
- Aural Foreign Body in Situ ForDocument3 pagesAural Foreign Body in Situ ForwilliamPas encore d'évaluation
- Vervet Monkey Eye Pressure Study Using PhencyclidineDocument3 pagesVervet Monkey Eye Pressure Study Using PhencyclidineRommel Barbosa MonteiroPas encore d'évaluation
- Warrants Say Bassett Man Fatally Shot His Sister's Boyfriend To Protect Her From AssaultDocument3 pagesWarrants Say Bassett Man Fatally Shot His Sister's Boyfriend To Protect Her From AssaultWSETPas encore d'évaluation
- NC Woman Files Lawsuit Against Liberty University, Claims She Got Several RobocallsDocument13 pagesNC Woman Files Lawsuit Against Liberty University, Claims She Got Several RobocallsWSETPas encore d'évaluation
- WARRANTS - Woman Charged in Campbell County ShootingDocument2 pagesWARRANTS - Woman Charged in Campbell County ShootingWSET100% (1)
- Final Letter To Pres. Biden Re Presidential Budget 0Document2 pagesFinal Letter To Pres. Biden Re Presidential Budget 0WSETPas encore d'évaluation
- Sen. Newman, Obenshain Make Statement Ahead of Report On Investigation of OSICDocument6 pagesSen. Newman, Obenshain Make Statement Ahead of Report On Investigation of OSICWSETPas encore d'évaluation
- LFD Captain Files Lawsuit Against City Officials For Civil Rights ViolationsDocument2 pagesLFD Captain Files Lawsuit Against City Officials For Civil Rights ViolationsWSETPas encore d'évaluation
- Former Virginia Tech Soccer Player Sues CoachDocument13 pagesFormer Virginia Tech Soccer Player Sues CoachWSETPas encore d'évaluation
- 1 Suspect Faces 3 Additional Charges Following Amherst Co. ShootingDocument3 pages1 Suspect Faces 3 Additional Charges Following Amherst Co. ShootingWSETPas encore d'évaluation
- 2 Dead After Bedford County ShootingDocument5 pages2 Dead After Bedford County ShootingWSETPas encore d'évaluation
- FOIA of All ComplaintsDocument710 pagesFOIA of All ComplaintsWSETPas encore d'évaluation
- Newman Calls Northam's Proposal of Parole Board Investigation 'Deep Conflict of Interest'Document1 pageNewman Calls Northam's Proposal of Parole Board Investigation 'Deep Conflict of Interest'WSETPas encore d'évaluation
- Court Documents Detail How Deputies Found Victim in Franklin County Alleged Murder-SuicideDocument3 pagesCourt Documents Detail How Deputies Found Victim in Franklin County Alleged Murder-SuicideWSETPas encore d'évaluation
- Warrant For December 2020 Lynchburg HomicideDocument1 pageWarrant For December 2020 Lynchburg HomicideWSETPas encore d'évaluation
- Virginia COVID-19 Dashboard On Friday, March 19, 2021Document1 pageVirginia COVID-19 Dashboard On Friday, March 19, 2021WSETPas encore d'évaluation
- VMI Interim ReportDocument102 pagesVMI Interim ReportWSLSPas encore d'évaluation
- Franklin County Public Schools Grade Distribution Feb 2021Document5 pagesFranklin County Public Schools Grade Distribution Feb 2021Sara Grace ToddPas encore d'évaluation
- Moschetti Combined and ReducedDocument13 pagesMoschetti Combined and ReducedWSETPas encore d'évaluation
- Statement of FactsDocument6 pagesStatement of FactsWSETPas encore d'évaluation
- Montgomery Co. Man Faces Charged For Taking Part in US Capitol RiotDocument9 pagesMontgomery Co. Man Faces Charged For Taking Part in US Capitol RiotWSETPas encore d'évaluation
- Notice of Violation - Liberty UniversityDocument8 pagesNotice of Violation - Liberty UniversityJeff WilliamsonPas encore d'évaluation
- Gov. Ralph Northam's Amended Executive Order #72Document19 pagesGov. Ralph Northam's Amended Executive Order #72WSETPas encore d'évaluation
- Documents Detail How Police Found Body of 18-Year-Old Roanoke Woman in RiverDocument8 pagesDocuments Detail How Police Found Body of 18-Year-Old Roanoke Woman in RiverWSETPas encore d'évaluation
- Forest Couple Says Squatters Refuse To Leave Their HomeDocument19 pagesForest Couple Says Squatters Refuse To Leave Their HomeElizabethRiebe-ThomasPas encore d'évaluation
- Derrick Thompson DocumentsDocument6 pagesDerrick Thompson DocumentsWSETPas encore d'évaluation
- Fracker Warrant ApplicationDocument20 pagesFracker Warrant ApplicationJ Rohrlich100% (1)
- Virginia State Legislature Letter To Vice President PenceDocument2 pagesVirginia State Legislature Letter To Vice President PenceWSETPas encore d'évaluation
- 2 Men Charged After Martinsville Restaurant ShootingDocument7 pages2 Men Charged After Martinsville Restaurant ShootingWSETPas encore d'évaluation
- April 14, 2020, Court of Appeals DecisionDocument22 pagesApril 14, 2020, Court of Appeals DecisionWSETPas encore d'évaluation
- Family of Lynchburg Murder Victim Speaks Out After Convicted Killer Granted ParoleDocument4 pagesFamily of Lynchburg Murder Victim Speaks Out After Convicted Killer Granted ParoleWSETPas encore d'évaluation
- Family of Lynchburg Murder Victim Speaks Out After Convicted Killer Granted ParoleDocument4 pagesFamily of Lynchburg Murder Victim Speaks Out After Convicted Killer Granted ParoleWSETPas encore d'évaluation
- Comparison OF Bronchoalveolar Lavage Cytology and Biopsy in Lung MalignancyDocument5 pagesComparison OF Bronchoalveolar Lavage Cytology and Biopsy in Lung MalignancyDyahSavitriKusumoningtyasPas encore d'évaluation
- Recurrence of Pulmonary Intravascular BRDocument79 pagesRecurrence of Pulmonary Intravascular BRMikmik bay BayPas encore d'évaluation
- Pediatric-Rigid BronchoscopeDocument4 pagesPediatric-Rigid BronchoscopeAli HadiPas encore d'évaluation
- EndoscopeDocument12 pagesEndoscopemamjoud mustaphaPas encore d'évaluation
- CPT and ICD-10 codes for operative reportDocument11 pagesCPT and ICD-10 codes for operative reportmike_steven12Pas encore d'évaluation
- One Lung Ventilation: Llalando L. Austin Ii, MHSC, Aa-C, RRT Nova Southeastern UniversityDocument47 pagesOne Lung Ventilation: Llalando L. Austin Ii, MHSC, Aa-C, RRT Nova Southeastern UniversityZulkarnainBustamam100% (1)
- Kewenangan Klinis Spesialis THTDocument8 pagesKewenangan Klinis Spesialis THTANONIM100% (1)
- Wheezing Infant GuidelineDocument18 pagesWheezing Infant GuidelineLoredana GavrilescuPas encore d'évaluation
- AsdfDocument2 pagesAsdfMagma SanggiriPas encore d'évaluation
- Competency Appraisal - Diagnostic TestsDocument7 pagesCompetency Appraisal - Diagnostic TestsMj BrionesPas encore d'évaluation
- E Posters PDFDocument349 pagesE Posters PDFpriyadikkalaPas encore d'évaluation
- 11 Lung CancerDocument30 pages11 Lung CancerMuhammadPas encore d'évaluation
- OxygenationDocument57 pagesOxygenationscent0730100% (3)
- 09 - Instructions For Use - BF220 Series - User's Manual of HiVisu - BF220 Series Single-Use Digital Flexible Bronchoscope - A3Document25 pages09 - Instructions For Use - BF220 Series - User's Manual of HiVisu - BF220 Series Single-Use Digital Flexible Bronchoscope - A3Владислав АлександровичPas encore d'évaluation
- Seminar ReportDocument27 pagesSeminar ReportanarghyavPas encore d'évaluation
- Manujet Jet VentilatorDocument2 pagesManujet Jet VentilatorRajat MukherjeePas encore d'évaluation
- Stridor - Diagnosis & ManagementDocument54 pagesStridor - Diagnosis & ManagementNaseema273Pas encore d'évaluation
- UworldDocument721 pagesUworldIrish Eunice FelixPas encore d'évaluation
- CPC Mock 5-QDocument21 pagesCPC Mock 5-Qneerajcmi100% (2)
- Torax Karl StorzDocument314 pagesTorax Karl StorzLuis Francisco Gonzalez MolinaPas encore d'évaluation
- Eye, E.N.T. & Dental AnaesthesiaDocument22 pagesEye, E.N.T. & Dental AnaesthesiawellawalalasithPas encore d'évaluation
- NCM 112 Care of Clients With Problems in Oxygenation, Fluid and Electrolytes, Infectious, Inflammatory & Immunologic ReactionDocument52 pagesNCM 112 Care of Clients With Problems in Oxygenation, Fluid and Electrolytes, Infectious, Inflammatory & Immunologic ReactionJIMENEZ, TRISHA MARIE D.100% (1)
- Questions Med SurgDocument6 pagesQuestions Med SurgMyung Dae ChoiPas encore d'évaluation
- @anesthesia Books 2012 Clinical PDFDocument566 pages@anesthesia Books 2012 Clinical PDFRicardoPas encore d'évaluation
- Biomedical Equipment & IEC 60601Document169 pagesBiomedical Equipment & IEC 60601nebiyu mulugetaPas encore d'évaluation
- Videoscope System: OlympusDocument8 pagesVideoscope System: OlympusjoanPas encore d'évaluation
- Diagnostic Imaging and Procedures for Respiratory DiseaseDocument41 pagesDiagnostic Imaging and Procedures for Respiratory DiseaseVio Mincu100% (1)
- Jeopardy Game - BurnsDocument42 pagesJeopardy Game - BurnsPC NPas encore d'évaluation
- Dept. of Pulmonology expertise in lung careDocument7 pagesDept. of Pulmonology expertise in lung carerohit6varma-4Pas encore d'évaluation
- ENT InstrumentsDocument9 pagesENT InstrumentsMuhammad Farrukh ul IslamPas encore d'évaluation
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionD'EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionÉvaluation : 4 sur 5 étoiles4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityD'EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityÉvaluation : 4 sur 5 étoiles4/5 (13)
- The Comfort of Crows: A Backyard YearD'EverandThe Comfort of Crows: A Backyard YearÉvaluation : 4.5 sur 5 étoiles4.5/5 (23)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsD'EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsÉvaluation : 3.5 sur 5 étoiles3.5/5 (3)
- Why We Die: The New Science of Aging and the Quest for ImmortalityD'EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityÉvaluation : 3.5 sur 5 étoiles3.5/5 (2)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedD'EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedÉvaluation : 5 sur 5 étoiles5/5 (78)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeD'EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BePas encore d'évaluation
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsD'EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsÉvaluation : 5 sur 5 étoiles5/5 (1)
- Techniques Exercises And Tricks For Memory ImprovementD'EverandTechniques Exercises And Tricks For Memory ImprovementÉvaluation : 4.5 sur 5 étoiles4.5/5 (40)
- The Obesity Code: Unlocking the Secrets of Weight LossD'EverandThe Obesity Code: Unlocking the Secrets of Weight LossÉvaluation : 5 sur 5 étoiles5/5 (4)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisD'EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisÉvaluation : 4 sur 5 étoiles4/5 (1)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisD'EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisÉvaluation : 5 sur 5 étoiles5/5 (8)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsD'EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsÉvaluation : 4.5 sur 5 étoiles4.5/5 (169)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingD'EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (33)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsD'EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsPas encore d'évaluation
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingD'EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingÉvaluation : 5 sur 5 étoiles5/5 (5)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.D'EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Évaluation : 4.5 sur 5 étoiles4.5/5 (110)
- The Ultimate Guide To Memory Improvement TechniquesD'EverandThe Ultimate Guide To Memory Improvement TechniquesÉvaluation : 5 sur 5 étoiles5/5 (34)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaD'EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeD'EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeÉvaluation : 4.5 sur 5 étoiles4.5/5 (253)
- The Happiness Trap: How to Stop Struggling and Start LivingD'EverandThe Happiness Trap: How to Stop Struggling and Start LivingÉvaluation : 4 sur 5 étoiles4/5 (1)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsD'EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsPas encore d'évaluation
- Recovering from Emotionally Immature Parents: Practical Tools to Establish Boundaries and Reclaim Your Emotional AutonomyD'EverandRecovering from Emotionally Immature Parents: Practical Tools to Establish Boundaries and Reclaim Your Emotional AutonomyÉvaluation : 4.5 sur 5 étoiles4.5/5 (201)
- The Tennis Partner: A Doctor's Story of Friendship and LossD'EverandThe Tennis Partner: A Doctor's Story of Friendship and LossÉvaluation : 4.5 sur 5 étoiles4.5/5 (4)