Académique Documents
Professionnel Documents
Culture Documents
The Genetic Epidemiology of Irrational F
Transféré par
shahymossalamCopyright
Formats disponibles
Partager ce document
Partager ou intégrer le document
Avez-vous trouvé ce document utile ?
Ce contenu est-il inapproprié ?
Signaler ce documentDroits d'auteur :
Formats disponibles
The Genetic Epidemiology of Irrational F
Transféré par
shahymossalamDroits d'auteur :
Formats disponibles
ORIGINAL ARTICLE
The Genetic Epidemiology of Irrational Fears
and Phobias in Men
Kenneth S. Kendler, MD; John Myers, MS; Carol A. Prescott, PhD; Michael C. Neale, PhD
Background: Much of our knowledge of the role of ge- phobias. All 5 phobia subtypes aggregate within twin-
netic factors in the etiology of phobias comes from one pairs. This aggregation is due largely or solely to genetic
population-based sample of female twins. We examined factors with heritability of liabilities ranging from 25%
the sources of individual differences in the risks for pho- to 37%. Multivariate analysis revealed a common ge-
bias and their associated irrational fears in male twins. netic factor, genetic factors specific to each subtype, and
a common familial-environmental factor.
Methods: In personal interviews with both members of
1198 male-male twin pairs (707 monozygotic [MZ] and Conclusions: In male subjects, genetic risk factors,
491 dizygotic [DZ]) ascertained from a population- which are partially common across all subtypes and
based registry, we assessed the lifetime history of agora- partially subtype specific, play a moderate role in the
phobia and social, animal, situational, and blood/injury etiology of phobias and their associated irrational fears.
phobias as well as their associated irrational fears. Twin Family environment probably has an impact on risk for
resemblance was assessed by means of probandwise con- agoraphobia and social phobia. The genetic liability to
cordance, odds ratios, tetrachoric correlations, and uni- blood/injury phobias is not distinct from those of the
variate and multivariate biometrical model fitting. more typical phobias.
Results: The suggestive results obtained by analysis of
phobias only were supported by analyzing both fears and Arch Gen Psychiatry. 2001;58:257-265
F
AMILY STUDIES suggest that measurement error suggested that the re-
phobias are familial,1-6 but sults for these phobia subtypes were simi-
cannot clarify the origin of lar to those for the others (ie, the familial
this family resemblance. Twin transmission due solely to genetic factors).
studies of self-reported fears Third, high levels of comorbidity were seen
consistently have suggested a significant role between the phobia subtypes.15 Contrary to
for genetic factors.7-11 By contrast, twin stud- results from family studies,4 the best-
ies of clinically defined phobias have, with fitting multivariate model suggested com-
one exception, suffered from very small mon genetic and individual-specific envi-
samples sizes with resultant low power to ronmental factors that influenced risk for
discriminate alternative models of familial all phobia subtypes, as well as genetic and
transmission.12-14 This exception is our pre- environmental factors unique to each sub-
vious study of phobias in female-female type. However, these analyses did not in-
twins from the Virginia Twin Registry.15-17 clude BiP, which was assessed at a later wave.
These reports examined 5 types of pho- Blood/injury phobia differs from typical pho-
bias—agoraphobia (AgP), social phobia bias,18 where exposure to phobic stimuli (eg,
From the Virginia Institute for (SoP), animal phobia (AnP), situational pho- snakes, heights, and public speaking) usu-
Psychiatric and Behavioral bia (SiP), and blood/injury phobia (BiP)— ally produces increased sympathetic activ-
Genetics (Drs Kendler, and reached the following conclusions. First, ity (eg, tachycardia, increased blood pres-
Prescott, and Neale and all phobia subtypes are moderately famil- sure, sweating, and flushing). By contrast,
Mr Myers) and the ial. Second, familial aggregation of AgP, SoP, in individuals with BiP, exposure to pho-
Departments of Psychiatry and AnP is due to genetic factors. For SiP bic stimuli (eg, needles and blood) usually
(Drs Kendler, Prescott, and
Neale and Mr Myers) and
and BiP, results based on our first assess- increases parasympathetic activity (eg, bra-
Human Genetics (Drs Kendler ment15,16 suggested that twin resemblance dycardia, hypotension, pallor, and fainting).
and Neale), Medical College might result from familial-environmental Given these differences, would the genetic
of Virginia of Virginia factors. However, when our analyses in- and environmental risk factors for BiP be dis-
Commonwealth University, cluded a second assessment interview,17 the tinct from those for the other phobia sub-
Richmond. added power obtained through control of types?
(REPRINTED) ARCH GEN PSYCHIATRY/ VOL 58, MAR 2001 WWW.ARCHGENPSYCHIATRY.COM
257
Downloaded from www.archgenpsychiatry.com at Virginia Commonwealth University, on August 21, 2007
©2001 American Medical Association. All rights reserved.
SUBJECTS AND METHODS performed using a discriminant function analysis based on
6 standard zygosity questions. The algorithm was devel-
SAMPLE AND ASSESSMENT PROCEDURES oped on 227 twin pairs who underwent genotyping using
8 or more highly polymorphic DNA markers.19
This report is based on data from the second wave of in- We assessed a lifetime history of phobias with an ad-
terviews in our study of adult twins from the Virginia Twin aptation of the phobic disorders section of the Diagnostic
Registry (now part of the Mid-Atlantic Twin Registry), de- Interview Schedule (DIS) Version III-A.15,20 The 22 specific
tails of which have been outlined previously.19 Briefly, twins individual fears that were assessed are outlined in Table 1.
were eligible for participation if one or both members were We also asked respondents “Is there anything else you’ve been
successfully matched and if they were white, a member of unreasonably terrified to do or be near?” If any phobia de-
a multiple birth that included at least 1 male, and born be- scribed in response to this question best belonged with 1 of
tween 1940 and 1974. Of 9417 eligible individuals for the the 5 specific subtypes, it was so treated. Other phobias men-
first wave, 6814 (72.4%) completed initial interviews. For tioned in response to this question (eg, fear of darkness) were
those who completed the initial interview, we recontacted included in our analysis of any phobia, but were not counted
them to schedule a second interview at least 1 year later. as belonging to a specific subtype.
Where possible, this interview was completed face-to-face In the DIS, to be considered a phobia, the fear must
(79.4% of sample). Of the eligible individuals, 5629 (82.6%) result in seeing a physician, taking medications, or report-
were successfully interviewed. To assess test-retest reli- ing that the fear or its avoidance “interfered with life or ac-
ability, 150 members of male-male twins were reinter- tivities a lot.” Given the low and variable rates of treat-
viewed a mean (± SD) of 4.4±1.1 weeks after their initial ment seeking for phobias,21 we defined phobias solely
interview. through a modification of the third criterion, objective im-
The current report is based on 1198 male-male pairs pact of the fear on respondent behavior. In contrast to the
(707 monozygotic [MZ] and 491 dizygotic [DZ]) with com- DIS, where the respondent makes the judgment about fear-
plete data on irrational fears and phobias from the second- associated interference, in our interview, the interviewer
wave interview and 544 interviewed individual twins (254 made this assessment.
from MZ and 290 from DZ pairs) with complete data whose
co-twins did not complete a second-wave interview. STATISTICAL ANALYSIS
At the second-wave interview (1994 through 1998),
subjects were aged 20 to 58 years (mean ± SD, 36.8 ± 9.1 The univariate and multivariate twin models used in this
years). Interviewers had a master’s degree in a mental health– report are described elsewhere.15,22 We assume that varia-
related field or a bachelor’s degree in this area plus 2 years tion in liability to phobias results from the following 3 sets
of clinical experience. Members of a twin pair were in- of factors: (1) additive genetic (A), which contribute twice
terviewed by different interviewers unaware of clinical as much to the correlation in MZ twins as DZ twins; (2)
information about the co-twin. Zygosity diagnosis was family or common environment (those familial factors such
In this report, using our recently studied sample of in the direction opposite that predicted. Controlling for
male-male twin pairs ascertained from the same regis- zygosity, twin pairs with more similar childhood environ-
try, we address the following questions: ments were significantly less likely to be concordant for
AnP (x21 =5.55; P=.02) and SiP (x21 =4.10; P=.04). Those
1. What are the sources of individual differences in
in frequent adult contact were significantly more likely to
risk for the 5 phobia subtypes in male twins?
be concordant for SiP (x21 =5.27; P=.02).
2. Do irrational fears without impairment reflect a
Short-term test-retest reliability for irrational fears and
milder form of the same liability dimensions as classic
phobias, as assessed by the coefficient and the tetrachoric
phobias? If so, will including such fears in the modeling
correlation, were modest to moderate (Table 2). With the
improve power and the ability to discriminate compet-
exception of social fears/SoP, irrational fears were more re-
ing models?
liably reported than phobias. The reliability of the assign-
3. What is the level of comorbidity among individual
ment of a phobia given an irrational fear was particularly
phobia subtypes in this population sample? To what degree
modest. Consistent with our previous results,17 individu-
do genetic and environmental common factors contribute
als may be more reliable at recalling irrational fears than
to the observed patterns of comorbidity, and will these com-
they are at reporting their behavioral consequences.
mon factors have less impact on the liability to BiP than on
the liability to the more typical phobia subtypes?
DESCRIPTION BY INDIVIDUAL FEAR
RESULTS Many more individuals endorsed an irrational fear than
met criteria for an associated phobia (Table 1). How-
TEST FOR BIASES AND RELIABILITY ever, this ratio differed widely. For example, although
46% of individuals who feared being in crowds met cri-
We performed 12 analyses predicting twin concordance teria for AgP, the parallel figures for fears of needles, giv-
for each phobia subtype and any phobias from the simi- ing a speech, and snakes were 18%, 15%, and 14%, re-
larity of their childhood environment and the frequency spectively. Table 1 also presents, within each of the phobia
of adult contact. Three were significant at the 5% level; 2, subtypes, the proportion of individuals who met crite-
(REPRINTED) ARCH GEN PSYCHIATRY/ VOL 58, MAR 2001 WWW.ARCHGENPSYCHIATRY.COM
258
Downloaded from www.archgenpsychiatry.com at Virginia Commonwealth University, on August 21, 2007
©2001 American Medical Association. All rights reserved.
as parental attitudes that are shared by members of a twin Likewise, the corresponding subset of the matrix of thresh-
pair) (C), which contribute equally to the correlation in olds is created. These matrices are then used to compute
MZ and DZ twins; and (3) individual specific environ- the log-likelihood of the observation in question. The log-
ment (E), which reflect environmental experiences not likelihoods of all cases are summed to obtain the log-
shared by members of a twin pair and therefore contribute likelihood of the sample, which is maximized using nu-
to differences between them in their phobia histories. merical optimization software. An advantage of this method
Our multivariate twin analyses decompose into ge- is that it reduces the possible impact of cooperation bias
netic and environmental sources the variance in phobia li- by using information on potential differences in the preva-
ability and the covariance in liability among different pho- lence of phobias in those twins with vs those without a co-
bia subtypes. We attempt, in these analyses, to explain the twin participating to obtain a better estimate of true preva-
correlations between the phobia subtypes as resulting from lences.
a small number of latent factors. Multivariate genetic analy- Because maximum likelihood analysis of raw ordinal
sis goes beyond traditional factor analysis in providing in- data does not provide an overall test of goodness of fit, we
sight into the causes of resemblance among variables. compare relative fits against the full model. Twice the dif-
Two alternative multivariate models that describe how ference in log-likelihood between the full model and sub-
genetic and environmental factors influence covariation are model tested yields a statistic that is asymptotically x2, with
tested. Genetic and environmental factors could influence degrees of freedom equal to the difference in the number
covariation through a single common pathway.23 By con- of parameters in both models. Alternative models are evalu-
trast, in the independent pathway model, genes and the ated for the optimal balance between explanatory power
environment contribute to covariation through separate and parsimony, which is operationalized by Akaike’s In-
genetic and environmental latent factors. formation Criterion (AIC).25,26
Having 5 phobia subtypes, two factors were poten- Because unreasonable fears are more common than
tially identifiable. However, we focused on single com- phobias, analysis including fears would have increased
mon factor models, because this was the approach used power.27 Such analysis would be appropriate if fears and
previously.15 The relationship between the common ge- phobias resulted from a single continuum of liability, a hy-
netic factor and BiP was evaluated by setting the connect- pothesis testable by the multiple-threshold model.28 For our
ing path to 0 and examining the change in fit. analyses, P indicates phobias only, and FP, fears and pho-
To use complete twin pairs and twins whose co-twin bias.
was not interviewed, we used an Mx option24 to fit models We tested the equal environment assumption that
by maximum likelihood. During optimization, trial values exposure of MZ and DZ twin pairs to environmental risk
of the parameters are used to generate a predicted covari- factors for fears and phobias was equally correlated by pre-
ance matrix and a matrix of thresholds. For any particular dicting twin concordance for phobias, controlling for
observation, the overall matrix is filtered to create a sub- zygosity by means of the similarity of environmental ex-
matrix matching those observations that are present. periences of the twins in childhood29 and adulthood.
ria for phobia based on each specific fear. The most com- sulted from both genetic and familial-environmental fac-
mon impairing fears for each subtype were being in crowds tors. When we tested the simpler AE and CE models in
for AgP, giving a speech for SoP, snakes for AnP, other these 2 phobias, they produced nearly identical fits. Table
high places for SiP, and dentists or hospitals for BiP. 4 presents results for the AE model. The CE model pro-
The most common phobia subtype was SiP, fol- duced the following estimates for c2 and e2: −0.29 and
lowed by SoP, BiP, AnP, and AgP. No significant differ- 0.71, respectively, for AgP, and 0.17 and 0.83, respec-
ences were seen in the prevalence of the phobia subtypes tively, for SoP. The E-only model, by contrast, fit more
or any phobia in MZ vs DZ twins (results not shown). poorly for both phobias. Although AgP and SoP aggre-
gated within twin pairs, we had no power to distinguish
TWIN RESEMBLANCE the degree to which this was due to genetic and/or en-
vironmental mechanisms.
Twin resemblance was seen for all 5 of the phobia sub- For AnP, SiP, BiP, and any phobia, c2 was esti-
types in MZ twins, with the odds ratios (ORs) ranging mated at 0 in the full model, indicating that twin resem-
from 2.30 for SoP to 4.64 for AnP (Table 3). In DZ twins, blance was ascribed entirely to genetic factors. In each
twin resemblance was seen for AgP, SoP, and AnP, but case, the AE model fit somewhat better than the CE
not for SiP or BiP. For all phobia subtypes as well as for model, with estimates of heritability ranging from 0.22
any phobia, the OR and tetrachoric correlations in MZ (for any phobia) to 0.35 (for AnP). The very wide confi-
twins exceeded those seen in DZ twins, suggesting the dence intervals (CIs) on these heritability estimates are
importance of genetic risk factors. noteworthy. Furthermore, using the more rigorous x2
difference test, we could not reject the CE against the
UNIVARIATE MODEL FITTING ACE model at any level approaching statistical signifi-
TO PHOBIAS ONLY cance. Indeed, even the test for familial aggregation of
phobias (the ACE vs E-only model) was significant only
Table 4 shows the results of model fitting for each of for AgP (x22 =6.05; P=.05), AnP (x22 =6.65; P=.04), SiP
the phobia subtypes and for any phobia. For AgP and SoP, (x 2 2 = 7.02; P = .03), and any phobia (x 2 2 = 10.83;
the full ACE model suggested that twin resemblance re- P=.004).
(REPRINTED) ARCH GEN PSYCHIATRY/ VOL 58, MAR 2001 WWW.ARCHGENPSYCHIATRY.COM
259
Downloaded from www.archgenpsychiatry.com at Virginia Commonwealth University, on August 21, 2007
©2001 American Medical Association. All rights reserved.
suggested for all 5 phobia subtypes that the familial ag-
Table 1. Specific Irrational Fears and Phobias gregation of phobia susceptibility was due solely to ge-
in 2940 Male Twins* netic factors. For each phobia/fear, AE was the best-fit
model, with estimates of the heritability of liability rang-
% of Sample (±SE)
Phobia, % of ing from 0.24 for SoFP to 0.43 for AgFP. Second, the sta-
Subtype, Item Irrational Fear Phobia Subtype ± SE tistical power with which we could reject alternative mod-
Agoraphobia els was substantially greater. Using the x2 difference test,
Going out of house alone 1.6 ± 0.2 0.6 ± 0.1 15.3 ± 3.3 we could reject the CE model against the ACE model at
Being in crowds 7.2 ± 0.5 3.3 ± 0.3 83.1 ± 3.5 or near the 5% level for the following 4 of the 5 fear/
Being in open spaces 0.4 ± 0.1 0.3 ± 0.1 8.5 ± 2.6 phobia subtypes: AgFP (x 2 1 = 3.64; P = .06), AnFP
1 or more items 8.6 ± 0.5 4.0 ± 0.4 100.0
(x21 =11.87; P,.001), SiFP (x21 =8.09; P=.004), and BiFP
Social phobia
Meeting new people 5.3 ± 0.4 1.4 ± 0.2 21.6 ± 3.0
(x21 = 3.21; P = .07). For all fears/phobias, we could re-
Giving a speech 29.5 ± 0.8 4.4 ± 0.4 70.7 ± 3.4 ject the E only (or no familial transmission model) with
Using public bathrooms 4.4 ± 0.4 1.3 ± 0.2 20.1 ± 3.0 confidence, ie, AgFP (x 2 2 = 21.49; P,.001), SoFP
Eating in public 1.4 ± 0.2 0.6 ± 0.2 10.3 ± 2.2 (x22 =22.97; P,.001), AnFP (x22 =42.17; P,.001), SiFP
1 or more items 32.7 ± 0.9 6.3 ± 0.5 100.0 (x22 = 34.32; P,.001), and BiFP (x22 = 25.30; P,.001).
Animal phobia Third, the CIs around the parameter estimates were con-
Spiders 7.9 ± 0.5 1.1 ± 0.2 21.7 ± 3.3
Bugs 2.5 ± 0.3 0.4 ± 0.1 8.6 ± 2.3
siderably narrower when we considered both fears and
Mice 1.6 ± 0.2 0.2 ± 0.1 3.3 ± 1.5 phobias in the model fitting compared with phobias alone.
Snakes 20.0 ± 0.7 2.9 ± 0.3 55.9 ± 4.0
Bats 2.2 ± 0.3 0.2 ± 0.1 4.6 ± 1.7 COMORBIDITY AMONG PHOBIA SUBTYPES
Other animals 3.9 ± 0.4 1.2 ± 0.2 23.0 ± 3.4 AND MULTIVARIATE MODEL FITTING
1 or more items 28.3 ± 0.8 5.2 ± 0.4 100.0
Situational phobia
Substantial comorbidity exists among all combinations
Tunnels 3.5 ± 0.3 0.5 ± 0.1 5.8 ± 1.4
Other closed places 9.1 ± 0.5 2.3 ± 0.3 24.3 ± 2.6 of the phobia subtypes (Table 6). As measured by OR
Bridges 4.1 ± 0.4 0.9 ± 0.2 9.1 ± 1.7 or tetrachoric correlations, the highest comorbidity is seen
Airplanes 8.0 ± 0.5 2.0 ± 0.3 21.4 ± 2.5 between AgP and SoP, followed by SoP and BiP. The pat-
Other high places 18.3 ± 0.7 4.8 ± 0.4 50.4 ± 3.0 tern of comorbidity of BiP is similar to that seen with more
1 or more items 31.2 ± 0.9 9.4 ± 0.5 100.0 “typical” phobias.
Blood/injury phobia
Because of greater statistical power and stability of
Sight of blood 4.4 ± 0.4 0.6 ± 0.2 11.3 ± 2.4
Needles or injections 11.1 ± 0.6 2.0 ± 0.3 34.5 ± 3.7
estimates, we performed multivariate model fitting with
Dentists or hospitals 6.9 ± 0.5 2.5 ± 0.3 43.7 ± 3.8 fears and phobias, the results of which are outlined in
Certain diseases such 9.4 ± 0.5 1.6 ± 0.2 27.4 ± 3.4 Table 7. Model 1 was the full independent pathway
as AIDs or cancer model with the A, C, and E common factors as well as
1 or more items 23.3 ± 0.8 5.7 ± 0.4 100.0 the A, C, and E factors specific to each phobia subtype.
When we tried to simplify this to a common pathway
*AIDS indicates acquired immunodeficiency syndrome.
model, the fit deteriorated substantially, and the AIC in-
creased. Therefore, in subsequent models, we set to 0,
UNIVARIATE MODEL FITTING in turn, the C common factor (model 3), the A common
TO FEARS AND PHOBIAS factor (model 4), the E common factor (model 5), the
phobia-specific C paths (model 6), and the phobia-
We began by testing with the multiple threshold model28 specific A paths (model 7). The AIC improved only for
the assumption that irrational fears and phobias repre- model 6. Indeed, the fit of the model was unchanged when
sented differing points on a single continuum of liabil- constraining to zero C paths unique to each phobia.
ity. Although none of the results for the 5 phobia sub- We then tested the relationship between the ge-
types, examined separately in MZ and DZ twins, were netic risk factors for BiFP and the more typical phobias.
statistically significant, the results for any phobia were Starting with model 6, we constrained to 0 the path from
significant in both twin groups (MZ, x25 = 80.0; P,.001; the common genetic factor to BiFP, thereby forcing all
DZ, x25 =67.7; P,.001). Therefore, we proceeded with genetic risk for BiFP to be independent of the other pho-
model fitting using the trivariate classification of unaf- bia subtypes. This model fit substantially more poorly than
fected, fear only, and phobia for the 5 specific subtypes model 6, with a deterioration of 6.5 x2 units (P=.01).
of fears and phobias only. The test-retest reliability for Parameter estimates for the best-fit model 6 are
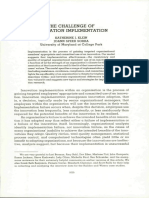
this trichotomy is shown in Table 2. seen in the Figure and Table 8. Five results are note-
The magnitude of the polychoric correlations for worthy. First, contrary to the hypothesis that the
fears/phobias in MZ and DZ twins (Table 3) are gener- genetic risk factors for BiFP are distinct from those for
ally similar to those seen with phobias only (although the more typical phobias, BiFP actually had the highest
there are some exceptions, eg, AgP). However, as ex- loading on the common genetic factor. Second, the
pected, the SEs of these correlations are substantially best-fit model also contained genetic risk factors spe-
smaller than those seen with phobias alone. cific to each phobia subtype. These genetic-specific fac-
The pattern of modeling results for fears and pho- tors were most important for SoFP, AnFP, and SiFP.
bias (Table 5) differed from that found with phobias Third, unlike the univariate analysis for fears/phobias
alone in 3 important ways. First, the full or ACE model (but more like the univariate analyses for phobias
(REPRINTED) ARCH GEN PSYCHIATRY/ VOL 58, MAR 2001 WWW.ARCHGENPSYCHIATRY.COM
260
Downloaded from www.archgenpsychiatry.com at Virginia Commonwealth University, on August 21, 2007
©2001 American Medical Association. All rights reserved.
Table 2. Test-Retest Reliability of Irrational Fears, Phobias, and Phobias for 150 Subjects Who Admit to Fears*
Phobia
Fear† Phobia† Fear-Phobia Dimension‡ (for Those Having Fear)†§
Tetrachoric Tetrachoric Polychoric Tetrachoric
Subtype k Correlation k Correlation Weighted k Correlation k Correlation
Agoraphobia 0.56 (0.28-0.85) 0.88 (0.60-0.98) 0.27 (−0.17-0.71) 0.72 (0.04-0.97) 0.48 (0.23-0.73) 0.86 (0.60-0.96) ... ...
Social phobia 0.35 (0.20-0.51) 0.60 (0.36-0.78) 0.37 (0.05-0.69) 0.76 (0.34-0.95) 0.36 (0.21-0.51) 0.64 (0.44-0.79) 0.31 (−0.12-0.74) 0.51 (−0.20-0.90)
Animal 0.58 (0.44-0.71) 0.80 (0.65-0.90) 0.17 (−0.09-0.44) 0.43 (−0.07-0.79) 0.50 (0.37-0.62) 0.70 (0.54-0.82) 0.14 (−0.20-0.48) 0.29 (−0.35-0.78)
phobia
Situational 0.58 (0.44-0.73) 0.82 (0.66-0.91) 0.35 (0.09-0.60) 0.66 (0.31-0.88) 0.52 (0.40-0.64) 0.78 (0.64-0.88) 0.16 (−0.19-0.51) 0.26 (−0.31-0.71)
phobia
Blood/injury 0.60 (0.45-0.76) 0.84 (0.67-0.93) 0.21 (−0.08-0.50) 0.50 (−0.01-0.83) 0.51 (0.37-0.65) 0.76 (0.59-0.87) 0.08 (−0.35-0.52) 0.15 (−0.53-0.74)
phobia
Any phobia 0.51 (0.37-0.66) 0.76 (0.59-0.87) 0.36 (0.18-0.53) 0.58 (0.33-0.77) 0.45 (0.33-0.56) 0.67 (0.52-0.78) 0.30 (0.08-0.51) 0.46 (0.12-0.72)
*Parenthetical data are 95% confidence intervals.
†Zero indicates none; 1, fear.
‡Zero indicates none; 1, fear; and 2, phobia.
§For agoraphobia, sample was too small for stable estimate.
Table 3. Prevalence and Measures of Similarity for Phobias in MZ and DZ Male-Male Twin Pairs*
MZ Pairs (707 Pairs) DZ Pairs (491 Pairs)
Fears and Fears and
Phobias Phobias Phobias Phobias
Tetrachoric Polychoric Tetrachoric Polychoric
Probandwise Odds Ratio Correlation Correlation Probandwise Odds Ratio Correlation Correlation
Phobia Prevalence Concordance (95% CI) (ASE) (ASE) Prevalence Concordance (95% CI) (ASE) (ASE)
Agoraphobia 0.035 0.122 4.29 0.320 (0.157) 0.435 (0.089) 0.050 0.122 2.93 0.252 (0.166) 0.169 (0.122)
(1.19-15.47) (0.81-10.58)
Social 0.067 0.126 2.30 0.208 (0.124) 0.249 (0.055) 0.062 0.098 1.73 0.132 (0.161) 0.129 (0.069)
(0.92-5.77) (0.50-6.07)
Animal 0.045 0.159 4.64 0.360 (0.133) 0.397 (0.053) 0.053 0.077 1.58 0.103 (0.181) 0.037 (0.075)
(1.65-13.01) (0.35-7.08)
Situational 0.093 0.212 3.09 0.314 (0.096) 0.343 (0.053) 0.095 0.065 0.64 −0.109 (0.143) 0.055 (0.068)
(1.60-5.96) (0.19-2.15)
Blood/injury 0.054 0.156 3.62 0.314 (0.125) 0.309 (0.061) 0.100 0.041 0.81 −0.043 (0.210) 0.120 (0.079)
(1.42-9.27) (0.11-6.27)
Any 0.217 0.313 1.93 0.224 (0.070) . . .† 0.209 0.244 1.30 0.087 (0.089) . . .†
(1.29-2.89) (0.77-2.17)
*MZ indicates monozygotic; DZ, dizygotic; CI, confidence interval; and ASE, asymptotic SE.
†Ellipses indicate results were not presented because multiple threshold model fit poorly.
alone), we found evidence of the impact of shared envi- Individual phobia subtypes and any phobia aggre-
ronment, but only in the form of a common factor. This gated within twin pairs. For AnP, SiP, BiP, and any pho-
common factor significantly affected only AgFP and bia, the best-fit model suggested that familial aggrega-
SoFP. Fourth, the best-fit model contained one com- tion was due solely to genetic factors with modest
mon E factor. That is, some environmental experiences heritabilities. For AgP and SoP, model fitting could not
that were unique to individual twins influence the gen- distinguish between genetic and familial-environmen-
eral risk for fears/phobias. This factor had highest load- tal sources of twin resemblance. For all the phobia sub-
ings on AgFP and SoFP. Finally, substantial specific E types, power was limited, and CIs for the parameter es-
loadings were seen for all subtypes, which would repre- timates were broad.
sent an admixture of measurement error and environ- Many twins in our sample reported irrational fears
mental experiences that predisposed uniquely to indi- without objective impact on their lives. Given our need
vidual phobia subtypes. for greater statistical power to resolve sources of indi-
vidual differences and the low reliability with which in-
COMMENT dividuals recalled whether the fears were impairing, we
applied the multiple-threshold model28 to a trichoto-
We addressed 3 questions about the genetic epidemiol- mous classification of all individuals into unaffected, fear
ogy of irrational fears and phobias in male-male twin pairs only, and phobia. Results from these analyses indicated
from a population-based registry. We examine these ques- that for all the phobia subtypes, the pattern of results
tions in turn. within MZ and DZ twins pairs were consistent with the
(REPRINTED) ARCH GEN PSYCHIATRY/ VOL 58, MAR 2001 WWW.ARCHGENPSYCHIATRY.COM
261
Downloaded from www.archgenpsychiatry.com at Virginia Commonwealth University, on August 21, 2007
©2001 American Medical Association. All rights reserved.
Table 4. Model-Fitting Results for Phobias in Male-Male Twin Pairs*
Parameter Estimates
Fit of Models† Full Best-Fit
Phobia ACE AE CE E a2 c2 e2 a2 95% CI e2 95% CI
Agoraphobia‡
x2 984.0 984.2 984.2 990.1 0.20 0.14 0.66 0.37 0.07-0.61 0.63 0.39-0.93
AIC ... −1.8§ −1.8§ 2.1 ... ... ... ... ... ... ...
Social‡
x2 1383.9 1383.9 1383.9 1386.9 0.11 0.08 0.81 0.20 0.00-0.41 0.80 0.59-1.00
AIC ... −2.0§ −2.0§ −1.0 ... ... ... ... ... ... ...
Animal
x2 1189.8 1189.8 1191.1 1196.4 0.35 0.00 0.65 0.35 0.09-0.58 0.65 0.42-0.91
AIC ... −2.0§ −0.7 2.6 ... ... ... ... ... ... ...
Situational
x2 1837.5 1837.5 1840.3 1844.5 0.25 0.00 0.75 0.25 0.07-0.43 0.75 0.57-0.93
AIC ... −2.0§ 0.8 3.0 ... ... ... ... ... ... ...
Blood/injury
x2 1282.8 1282.8 1284.2 1287.8 0.28 0.00 0.72 0.28 0.03-0.51 0.72 0.49-0.97
AIC ... −2.0§ −0.6 1.0 ... ... ... ... ... ... ...
Any
x2 3080.3 3080.3 3081.7 3091.1 0.22 0.00 0.78 0.22 0.09-0.34 0.78 0.66-0.91
AIC ... −2.0§ −0.6 6.8 ... ... ... ... ... ... ...
*A indicates additive genetic factors; C, family or common environment factors; E, individual specific environment factors; CI, confidence interval; and AIC,
Akaike’s Information Criterion.25 Analyses were based on 1198 complete twin pairs and 544 single twins.
†Degrees of freedom were 2937 for ACE, 2938 for AE and CE, and 2939 for E.
‡For these phobias, we present parameters from the AE model as the best fit, but the CE model also fit nearly as well, results of which are presented in the
“Univariate Model Fitting to Phobias Only” subsection of the “Results” section.
§Best-fit models by means of AIC.
Table 5. Model-Fitting Results for Fears and Phobias in Male-Male Twin Pairs*
Parameter Estimates
Fit of Models† Full Best-Fit
Phobia ACE AE CE E a2 c2 e2 a2 95% CI e2 95% CI
Agoraphobia
x2 2040.8 2040.8 2044.4 2062.3 0.43 0.00 0.57 0.43 0.26-0.59 0.57 0.41-0.74
AIC ... −2.0† 1.6 17.5 ... ... ... ... ... ... ...
Social
x2 4637.2 4637.2 4638.9 4660.1 0.24 0.00 0.76 0.24 0.15-0.34 0.76 0.66-0.85
AIC ... −2.0† −0.3 18.9 ... ... ... ... ... ... ...
Animal
x2 4249.1 4249.1 4261.0 4291.3 0.37 0.00 0.63 0.37 0.26-0.47 0.63 0.53-0.74
AIC ... −2.0† 9.9 38.2 ... ... ... ... ... ... ...
Situational
x2 4745.6 4745.6 4753.7 4779.9 0.31 0.00 0.69 0.31 0.21-0.40 0.69 0.60-0.79
AIC ... −2.0† 6.1 30.3 ... ... ... ... ... ... ...
Blood/injury
x2 3926.5 3926.5 3929.7 3951.8 0.30 0.00 0.70 0.30 0.19-0.41 0.70 0.59-0.81
AIC ... −2.0† 1.2 25.3 ... ... ... ... ... ... ...
*Abbreviations and degrees of freedom for fit of models are given in the first and second footnotes to Table 4. Analyses were based on 1198 complete twin
pairs and 544 single twins. Degrees of freedom for fit of models were as follows: ACE, 2936; AE, 2937; CE, 2937; and E, 2938.
†Best fit model(s) by means of AIC.25
hypothesis that fears were a milder manifestation of the best-fit model for all the phobia subtypes suggested that
same liability dimension that produced clinical pho- familial resemblance was due solely to genetic factors, again
bias. We found similar results in our female twins.17 with modest heritability estimates, but now with consid-
We repeated our analysis using this trichotomous erably smaller CIs.
classification, with results that were substantially clearer We recently fitted multiple threshold models to data
than those obtained for phobias alone. With the in- on fears and phobias from the previously studied female-
creased statistical power, evidence of familial-environ- female pairs17 to which our current results can be com-
mental effects on AgP and SoP disappeared. The pared usefully. We used a measurement model based on
(REPRINTED) ARCH GEN PSYCHIATRY/ VOL 58, MAR 2001 WWW.ARCHGENPSYCHIATRY.COM
262
Downloaded from www.archgenpsychiatry.com at Virginia Commonwealth University, on August 21, 2007
©2001 American Medical Association. All rights reserved.
Table 6. Tetrachoric Correlation and Odds Ratios Between Phobias*
Phobia Agoraphobia Social Phobia Animal Phobia Situational Phobia Blood/Injury Phobia
Agoraphobia 12.78 (8.51-19.18) 5.37 (3.32-8.70) 3.70 (2.40-5.68) 3.44 (2.05-5.78)
Social 0.61 (0.05) 4.59 (3.01-7.01) 3.83 (2.68-5.46) 5.89 (3.99-8.70)
Animal 0.40 (0.06) 0.38 (0.06) 3.81 (2.59-5.59) 5.20 (3.39-7.96)
Situational 0.33 (0.06) 0.36 (0.05) 0.35 (0.05) 4.40 (3.07-6.31)
Blood/injury 0.29 (0.07) 0.45 (0.05) 0.41 (0.06) 0.39 (0.05)
*Data in lower-left triangle are given as tetrachoric correlations (asymptotic SE); in upper-right triangle, odds ratios (95% confidence intervals).
Table 7. Multivariate Model-Fitting Results for Specific Fears/Phobias*
Model Fear/Phobia Common Factors Fear/Phobia Specific Factors Pathway x2 df AIC†
1 ACE ACE Independent 18 675.7 14 662 . . .‡
2 ACE ACE Common 18 714.9 14 671 21.2
3 AE ACE Independent 18 690.3 14 667 5.6
4 CE ACE Independent 18 703.3 14 667 17.6
5 AC ACE Independent 18 836.5 14 667 150.8
6 ACE AE Independent 18 675.7 14 667 −10.0
7 ACE CE Independent 18 686.9 14 667 1.2
*Abbreviations are given in the first footnote to Table 4.
†Explained in Akaike.25
‡No estimate of AIC possible for first or full model.
2 waves of interviews from which we can derive ex-
pected heritability from a single interview: for AgFP, 0.47; AC CC EC
for SoFP, 0.31; for AnFP, 0.27; for SiFP, 0.26; and for 0.47 0.48 – 0.12 0.50
BiFP, 0.32. These results, well within the 95% CIs ob- 0.36 0.22 0.03 0.65
tained in the male sample, suggest that the role of ge- 0.46 – 0.03 0.38
0.33 0.22 0.34 0.46
netic factors in liability to irrational fears and phobias are
probably similar in men and women.
Similar to other community samples,15,30 substan-
tial comorbidity was seen between phobia subtypes. Mul-
tivariate twin modeling is a powerful method to exam- Agoraphobia Social Animal Situational Blood/Injury
ine the contributions of genetic and environmental factors Phobia Phobia Phobia Phobia
to observed patterns of comorbidity. Given the higher test-
retest reliability and greater power and stability of pa- 0.15 0.62 0.36 0.59 0.39 0.70 0.42 0.76 0.25 0.70
rameter estimates associated with adding of informa- AS ES AS ES AS ES AS ES AS ES
tion on irrational fears, we included these along with
phobias in our multivariate analyses. The best-fit model
Results from the best-fitting multivariate genetic model for the subtypes of
contained 3 common factors (reflecting genetic and shared phobias (model 6). A indicates additive genetic; C, common or shared family
and unique environments) that influenced liability to all environment; E, individual specific environmental effects; subscript C, phobia
forms of phobia. In addition, each phobic subtype had common factors; and subscript S, additive genetic and individual-specific
evidence of genetic and unique environmental factors spe- environmental effects specific to each phobic subtype. Thus, AC refers to the
additive genetic common factor (additive genes that influence liability to all
cific to that phobia. phobia subtypes); CC, the shared environmental common factor; and ES,
The pattern of results we obtained was similar to that individual-specific environmental experiences that uniquely influence liability
in our previous multivariate analysis in women (which only to 1 phobia subtype. The magnitude of each path, as estimated using
model 6, is shown. Squaring these path or standardized partial regression
contained only 4 phobia subtypes)15 in 2 important ways. coefficients gives the proportion of variance in the observed variable
In both sexes, certain genetic factors influenced risk for accounted for by the latent factor.
all phobia subtypes, whereas others specifically influ-
enced risk for individual phobic subtypes. In both sexes,
the loadings of AnP on this common genetic factor were a significant impact on AgP and SoP. These results sug-
higher than those for the other typical phobias of AgP, gest that twin siblings shared some environmental ex-
SoP, and SiP. We also saw evidence that in men and periences in their family or community that influence risk
women, certain individual environmental experiences in- specifically for AgP and SoP. Second, the pattern of load-
creased risk nonspecifically for all phobic subtypes, ings for phobia-specific genetic factors differed between
whereas others were phobia-subtype specific in their im- the sexes. For example, we found in women much larger
pact. However, 2 differences are noteworthy. First, we contributions of phobia-specific genetic influences for AgP
found evidence in our multivariate analysis in men but than AnP, whereas in men the findings were reversed.
not in women of shared environmental effects that had Further research will be required to determine if these
(REPRINTED) ARCH GEN PSYCHIATRY/ VOL 58, MAR 2001 WWW.ARCHGENPSYCHIATRY.COM
263
Downloaded from www.archgenpsychiatry.com at Virginia Commonwealth University, on August 21, 2007
©2001 American Medical Association. All rights reserved.
Table 8. Sources of Variance in Liability to Individual Phobia Subtypes From Best-Fit Fear/Phobia Multivariate Model
Genetic Unique Environment
Shared Environment,
Fear/Phobia Common Specific Total Common Common Specific Total
Agoraphobia 0.11 0.02 0.13 0.23 0.25 0.39 0.64
Social 0.05 0.13 0.18 0.05 0.42 0.35 0.77
Animal 0.21 0.15 0.36 0.00 0.15 0.49 0.64
Situational 0.13 0.18 0.31 0.00 0.12 0.57 0.69
Blood/injury 0.22 0.06 0.28 0.01 0.21 0.50 0.71
and other differences seen in both sexes are substantive netic proportion of reliable variance) would be consid-
in nature or due to stochastic fluctuations in patterns of erably higher than those reported herein.
phobia resemblances in twin pairs.
Our multivariate analyses also permitted us to evalu- Accepted for publication October 10, 2000.
ate the hypothesis that the genetic risk factors for BiP are This work was supported by grants MH/AA-49492 and
distinct from those for the more typical phobia sub- MH-54150 and Research Scientist awards MH-01277 (Dr
types. Our results were inconsistent with this hypoth- Kendler) and MH-01458 (Dr Neale) from the National In-
esis. Indeed, BiP had the highest loading on the com- stitutes of Health, Bethesda, Md. We acknowledge the con-
mon genetic factor, and we could not set that path to 0 tribution of the Virginia Twin Registry, now part of the Mid-
without a substantial deterioration in fit. The more typi- Atlantic Twin Registry, to ascertainment of subjects for this
cal phobias and BiP probably share common early fear study. The Mid-Atlantic Twin Registry, directed by Linda
pathways that then diverge in their outflow to the hy- Corey, PhD, and Lenn Murrelle, PhD, has received support
pothalamus and autonomic pathways.31 These findings from the National Institutes of Health, the Carman Trust
suggest that genetic risk factors for phobias in men act (Richmond, Va), and the WM Keck (Los Angeles, Calif),
largely on the individual differences in the sensitivity of John Templeton (Radnor, Pa), and Robert Wood Johnson
those early fear pathways shared by BiP and the more typi- (Princeton, NJ) Foundations.
cal phobias. These data were collected under the direction of Patsy
These analyses should be considered in the context Waring, Sarah Woltz, MA, and Frank Butera, MS.
of 2 potential methodological limitations. First, our cri- Corresponding author and reprints: Kenneth S. Ken-
teria for phobias differ from those proposed in recent DSM dler, MD, Department of Psychiatry, Medical College of Vir-
editions.32,33 For example, our interviewer-based assess- ginia of Virginia Commonwealth University, 800 E Leigh
ment of impairment, although more objective, may pro- St, PO Box 980126, Richmond, VA 23298-0126.
duce a lower threshold for interference than the self-
report measure used in the DIS. Our definition may also
REFERENCES
be broader than that proposed in DSM-III-R criteria32 in
that we require objective impact on respondent behav-
ior rather than the significant interference with normal 1. Noyes R, Crowe RR, Harris EL, Hamra BJ, McChesney CM, Chaudhry DR. Re-
lationship between panic disorder and agoraphobia. Arch Gen Psychiatry. 1986;
routine in DSM-III-R. However, DSM-III-R would in- 43:227-232.
clude an unreasonable fear that produced marked dis- 2. Fyer AJ, Mannuzza S, Gallops MS, Martin LY, Aaronson C, Gorman JM, Liebo-
tress, whereas we did not. The Epidemiological Catch- witz MR, Klein DF. Familial transmission of simple phobias and fears: a prelimi-
ment Area screened for a more limited number of phobic nary report. Arch Gen Psychiatry. 1990;47:252-256.
stimuli (14 specific fears) and produced a lifetime preva- 3. Fyer AJ, Mannuzza S, Chapman TF, Liebowitz MR, Klein DF. A direct interview
family study of social phobia. Arch Gen Psychiatry. 1993;50:286-293.
lence for any phobia in men of 10.4%,30 about half of what 4. Fyer AJ, Mannuzza S, Chapman TF, Martin LY, Klein DF. Specificity in familial
we found in this study. By contrast, compared with our aggregation of phobic disorders. Arch Gen Psychiatry. 1995;52:564-573.
results, the National Comorbidity Study found much 5. Mannuzza S, Schneier FR, Chapman TF, Liebowitz MR, Klein DF, Fyer AJ. Gen-
higher rates of SoP in men (11.1%)34 and slightly lower eralized social phobia: reliability and validity. Arch Gen Psychiatry. 1995;52:230-
237.
rates of AgP (3.5%).
6. Stein MB, Chartier MJ, Hazen AL, Kozak MV, Tancer ME, Lander S, Furer P, Chu-
Second, a lifetime history of irrational fears and pho- baty D, Walker JR. A direct-interview family study of generalized social phobia.
bias was assessed in this study at a single point in time. Am J Psychiatry. 1998;155:90-97.
If uncorrelated in twin pairs, unreliability of measure- 7. Torgersen S. The nature and origin of common phobic fears. Br J Psychiatry.
ment is indistinguishable from the effects of true indi- 1979;134:343-351.
8. Phillips K, Fulker DW, Rose RJ. Path analysis of seven fear factors in adult twin
vidual specific environment in our twin models. Our and sibling pairs and their parents. Genet Epidemiol. 1987;4:345-355.
short-term retest reliability found most tetrachoric cor- 9. Rose RJ, Ditto WB. A developmental-genetic analysis of common fears from early
relations for fears and phobias ranging from 0.60 to 0.85. adolescence to early adulthood. Child Dev. 1983;54:361-368.
These results suggest that a substantial proportion of what 10. Rose RJ, Miller JZ, Pogue-Geile MF, Cardwell GF. Twin-family studies of com-
we call E in our models in fact represents unreliability mon fears and phobias. In: Gedda L, Parisi P, Nance WE, eds. Intelligence, Per-
sonality, and Development. New York, NY: Alan R Liss Inc; 1981:169-174. Twin
of measurement. If our twin models were corrected for Research; vol 3, part 69B.
this effect, as shown in the female sample,17 the esti- 11. Neale MC, Fulker DW. A bivariate path analysis of fear data on twins and their
mates of the heritability of liability to phobias (ie, the ge- parents. Acta Genet Med Gemellol (Roma). 1984;33:273-286.
(REPRINTED) ARCH GEN PSYCHIATRY/ VOL 58, MAR 2001 WWW.ARCHGENPSYCHIATRY.COM
264
Downloaded from www.archgenpsychiatry.com at Virginia Commonwealth University, on August 21, 2007
©2001 American Medical Association. All rights reserved.
12. Carey G, Gottesman II. Twin and family studies of anxiety, phobic and obsessive toms of depression: same genes, different environments? Arch Gen Psychiatry.
disorders. In: Klein DF, Rabkin JG, eds. Anxiety: New Research and Changing 1987;44:451-457.
Concepts. New York, NY: Raven Press; 1981:117-135. 24. Neale MC. Statistical Modelling with Mx. Richmond: Department of Psychiatry,
13. Torgersen S. Genetic factors in anxiety disorders. Arch Gen Psychiatry. 1983; Medical College of Virginia; 1991.
40:1085-1089. 25. Akaike H. Factor analysis and AIC. Psychometrika. 1987;52:317-332.
14. Skre I, Onstad S, Torgersen S, Lygren S, Kringlen E. A twin study of DSM-III-R 26. Williams LJ, Holahan PJ. Parsimony-based fit indices for multiple-indicator mod-
anxiety disorders. Acta Psychiatr Scand. 1993;88:85-92. els: do they work? Struct Equation Modeling. 1994;1:161-189.
15. Kendler KS, Neale MC, Kessler RC, Heath AC, Eaves LJ. The genetic epidemi- 27. Neale MC, Eaves LJ, Kendler KS. The power of the classical twin study to re-
ology of phobias in women: the interrelationship of agoraphobia, social pho- solve variation in threshold traits. Behav Genet. 1994;24:239-258.
bia, situational phobia, and simple phobia. Arch Gen Psychiatry. 1992;49:273- 28. Reich T, James JW, Morris CA. The use of multiple thresholds in determining the
281. mode of transmission of semi-continuous traits. Ann Hum Genet. 1972;36:163-184.
16. Neale MC, Walters EE, Eaves LJ, Kessler RC, Heath AC, Kendler KS. The genet- 29. Loehlin JC, Nichols RC. Heredity, Environment and Personality: A Study of 850
ics of blood-injury fears and phobias: a population-based twin study. Am J Med Sets of Twins. Austin: University of Texas Press; 1976.
Genet. 1994;54:326-334. 30. Eaton WW, Dryman A, Weissman MM. Panic and phobia. In: Robins LN, Regier
17. Kendler KS, Karkowski LM, Prescott CA. Fears and phobias: reliability and heri- DA, eds. Psychiatric Disorders in America: The Epidemiologic Catchment Area
tability. Psychol Med. 1999;29:539-553. Study. New York, NY: Free Press; 1991:155-179.
18. Marks IM. Blood-injury phobia: a review. Am J Psychiatry. 1988;145:1207- 31. LeDoux JE. The Emotional Brain: The Mysterious Underpinnings of Emotional
1213. Life. New York, NY: Simon & Schuster; 1996.
19. Kendler KS, Karkowski L, Neale MC, Prescott CA. Illicit psychoactive substance 32. American Psychiatric Association. Diagnostic and Statistical Manual of Mental
use, heavy use, abuse, and dependence in a US population-based sample of male Disorders, Revised Third Edition. Washington, DC: American Psychiatric Asso-
twins. Arch Gen Psychiatry. 2000;57:261-269. ciation; 1987.
20. Robins LN, Helzer JE. Diagnostic Interview Schedule (DIS): Version III-A. St Louis, 33. American Psychiatric Association. Diagnostic and Statistical Manual of Mental
Mo: Washington University School of Medicine; 1985. Disorders, Fourth Edition. Washington, DC: American Psychiatric Association;
21. Kessler RC, Olfson M, Berglund PA. Patterns and predictors of treatment con- 1994.
tact after first onset of psychiatric disorders. Am J Psychiatry. 1998;155:62-69. 34. Kessler RC, McGonagle KA, Zhao S, Nelson CB, Hughes M, Eshleman S, Wittchen
22. Kendler KS. Twin studies of psychiatric illness: current status and future direc- H-U, Kendler KS. Lifetime and 12-month prevalence of DSM-III-R psychiatric dis-
tions. Arch Gen Psychiatry. 1993;50:905-915. orders in the United States: results from the National Comorbidity Survey. Arch
23. Kendler KS, Heath AC, Martin NG, Eaves LJ. Symptoms of anxiety and symp- Gen Psychiatry. 1994;51:8-19.
(REPRINTED) ARCH GEN PSYCHIATRY/ VOL 58, MAR 2001 WWW.ARCHGENPSYCHIATRY.COM
265
Downloaded from www.archgenpsychiatry.com at Virginia Commonwealth University, on August 21, 2007
©2001 American Medical Association. All rights reserved.
Vous aimerez peut-être aussi
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Application of Computer in PharmacyDocument4 pagesApplication of Computer in Pharmacybryankachocho17Pas encore d'évaluation
- Mapping Customer Segments For Personal Financial ServicesDocument9 pagesMapping Customer Segments For Personal Financial ServicesNash BelfonPas encore d'évaluation
- Strategy Analysis & ChoiceDocument49 pagesStrategy Analysis & ChoiceA'del JummaPas encore d'évaluation
- Resource H Approaching The Literature Review PowerpointDocument16 pagesResource H Approaching The Literature Review PowerpointAnonymous XTL7o0tGo9Pas encore d'évaluation
- Class 9Document15 pagesClass 9Diya lizbeth josePas encore d'évaluation
- 10 EtDocument76 pages10 EtMajor LoonyPas encore d'évaluation
- (Alsaleh, Nada J.) Teaching Critical Thinking Skills - Literature ReviewDocument19 pages(Alsaleh, Nada J.) Teaching Critical Thinking Skills - Literature ReviewLailaPas encore d'évaluation
- World Psychiatry - October 2013Document100 pagesWorld Psychiatry - October 2013zokica5Pas encore d'évaluation
- Abstract:: Peer Reviewed - International Journal Vol-6, Issue-1, 2022 (IJEBAR)Document9 pagesAbstract:: Peer Reviewed - International Journal Vol-6, Issue-1, 2022 (IJEBAR)firdha salsabilaPas encore d'évaluation
- Zamoras Group Research About GAS StudentsDocument17 pagesZamoras Group Research About GAS StudentsLenard ZamoraPas encore d'évaluation
- Improving Projects Performance With Lean Construction: State of The Art, Applicability and ImpactsDocument9 pagesImproving Projects Performance With Lean Construction: State of The Art, Applicability and ImpactsCherryl Chrissie JamesPas encore d'évaluation
- Benefits of Online EducationDocument26 pagesBenefits of Online EducationJebjeb C. BrañaPas encore d'évaluation
- Three Decades of Game Based Learning in Science and Mathematics Education-An Integrated Bibliometric Analysis and Systematic ReviewDocument22 pagesThree Decades of Game Based Learning in Science and Mathematics Education-An Integrated Bibliometric Analysis and Systematic ReviewBruna SantosPas encore d'évaluation
- Visvesvaraya Technological University, BelagaviDocument67 pagesVisvesvaraya Technological University, BelagaviAKSHAYKUMAR JAMADARPas encore d'évaluation
- DD309 Tma 05Document10 pagesDD309 Tma 05papanombaPas encore d'évaluation
- Advocacy in The Customer Focused Enterprise - IBM PDFDocument28 pagesAdvocacy in The Customer Focused Enterprise - IBM PDFAlberto ConzPas encore d'évaluation
- OrganizingDocument46 pagesOrganizingViswajeet BiswalPas encore d'évaluation
- ArchanaDocument6 pagesArchanaArchana DeviPas encore d'évaluation
- Pilferage Control in HospitalsDocument4 pagesPilferage Control in HospitalsDr. Rakshit Solanki100% (3)
- Dr. Toppelberg's PositionDocument5 pagesDr. Toppelberg's PositionGabriela Simon-CereijidoPas encore d'évaluation
- Assessment TU6214Document3 pagesAssessment TU6214AWANGKU MUHAMMAD AFFIF OMAR BIN AWANG RADUANPas encore d'évaluation
- Final Banana Peel CrackerDocument8 pagesFinal Banana Peel CrackerChoy Concha Albasin Eugenio-MarzoPas encore d'évaluation
- 3M AnalysisDocument5 pages3M AnalysisAritra BanerjeePas encore d'évaluation
- A Study On Level of Satisfaction of Using Lenovo Laptop Among The College Students With Special Reference To ST 1Document88 pagesA Study On Level of Satisfaction of Using Lenovo Laptop Among The College Students With Special Reference To ST 1ganesan ganesanPas encore d'évaluation
- SEC6010 - Planning For Information SecurityDocument9 pagesSEC6010 - Planning For Information SecurityVenkata Pathi JaligamaPas encore d'évaluation
- Innovation Implementation: The Challenge ofDocument27 pagesInnovation Implementation: The Challenge ofMalik Atif ZamanPas encore d'évaluation
- Bank Loan Pitch Deck by SlidesgoDocument40 pagesBank Loan Pitch Deck by SlidesgoHaikal MahranPas encore d'évaluation
- Title: Impact of Leadership Styles On Performance Through The Mediating Role of Employee's MotivationDocument29 pagesTitle: Impact of Leadership Styles On Performance Through The Mediating Role of Employee's Motivationsardar hussainPas encore d'évaluation
- Sensory-Ethical Intratim - IsFp (The Peacemaker)Document2 pagesSensory-Ethical Intratim - IsFp (The Peacemaker)ochoajulie87Pas encore d'évaluation
- Good Versus Bad Teaching - NichollsDocument29 pagesGood Versus Bad Teaching - Nichollsapi-300172472Pas encore d'évaluation