Vous aimerez peut-être aussi
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Megalourethra: A Rare Clinical Entity: ReferencesDocument1 pageMegalourethra: A Rare Clinical Entity: Referencesdella psPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Yokoyama 2000Document5 pagesYokoyama 2000della psPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Cranberry EditorialDocument2 pagesCranberry EditorialKorina LimnioudiPas encore d'évaluation
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Congenital Scaphoid Megalourethra: Report of Two CasesDocument3 pagesCongenital Scaphoid Megalourethra: Report of Two Casesdella psPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Long-Term Outcomes and Risk Factors Associated With Acute Encephalitis in ChildrenDocument8 pagesLong-Term Outcomes and Risk Factors Associated With Acute Encephalitis in ChildrenNovia RambakPas encore d'évaluation
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Guay 2009Document33 pagesGuay 2009della psPas encore d'évaluation
- An Investigation of Dentists' Knowledge, Attitudes and Practices Towards HIV and Patients With Other Blood-Borne Viruses in South Cheshire, UKDocument6 pagesAn Investigation of Dentists' Knowledge, Attitudes and Practices Towards HIV and Patients With Other Blood-Borne Viruses in South Cheshire, UKdella psPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- JAMA. 2016 : in ReplyDocument3 pagesJAMA. 2016 : in Replydella psPas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Di Bianco 1989Document7 pagesDi Bianco 1989della psPas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Patfis AsmaDocument14 pagesPatfis Asmadella psPas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Epidemiology of Asthma: ReviewDocument5 pagesEpidemiology of Asthma: Reviewdella psPas encore d'évaluation
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Review ArticleDocument8 pagesReview Articledella psPas encore d'évaluation
- Loftus 2016Document8 pagesLoftus 2016della psPas encore d'évaluation
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Oxygen in The ICU Too Much of A Good Thing?: EditorialDocument2 pagesOxygen in The ICU Too Much of A Good Thing?: Editorialdella psPas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Girard Is 2016Document7 pagesGirard Is 2016della psPas encore d'évaluation
- Oxygen in The Critically Ill: Friend or Foe?: ReviewDocument7 pagesOxygen in The Critically Ill: Friend or Foe?: Reviewdella psPas encore d'évaluation
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Oxygen: Breath of Life or Kiss of DeathDocument2 pagesOxygen: Breath of Life or Kiss of Deathdella psPas encore d'évaluation
- Kal Let 2016Document17 pagesKal Let 2016della psPas encore d'évaluation
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Paradigms of Oxygen Therapy in Critically Ill PatientsDocument6 pagesParadigms of Oxygen Therapy in Critically Ill Patientsdella psPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Pan War 2016Document51 pagesPan War 2016della psPas encore d'évaluation
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Suzuki 2014Document9 pagesSuzuki 2014della psPas encore d'évaluation
- Helmer Horst 2016Document10 pagesHelmer Horst 2016della psPas encore d'évaluation
- Placental Disease and The Maternal Syndrome of Preeclampsia: Missing Links?Document10 pagesPlacental Disease and The Maternal Syndrome of Preeclampsia: Missing Links?della psPas encore d'évaluation
- PNPK PreEklampsia 2016Document7 pagesPNPK PreEklampsia 2016della psPas encore d'évaluation
- Caumes Et Al-2004-Journal of Travel Medicine PDFDocument3 pagesCaumes Et Al-2004-Journal of Travel Medicine PDFdella psPas encore d'évaluation
- Epidemiology of Asthma: ReviewDocument5 pagesEpidemiology of Asthma: Reviewdella psPas encore d'évaluation
- Renal Hemodynamics During Carbon Dioxide Pneumoperitoneum: An Experimental Study in PigsDocument5 pagesRenal Hemodynamics During Carbon Dioxide Pneumoperitoneum: An Experimental Study in Pigsdella psPas encore d'évaluation
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (120)
- Placental Origins of Preeclampsia: Challenging The Current HypothesisDocument7 pagesPlacental Origins of Preeclampsia: Challenging The Current Hypothesisdella psPas encore d'évaluation
- Intermittent Low Dose Digoxin May Be Effective and Safe in Patients With Chronic Heart Failure Undergoing Maintenance HemodialysisDocument6 pagesIntermittent Low Dose Digoxin May Be Effective and Safe in Patients With Chronic Heart Failure Undergoing Maintenance Hemodialysisdella psPas encore d'évaluation
- Nursing Care of The Child With Respiratory DisordersDocument31 pagesNursing Care of The Child With Respiratory DisordersCnette S. LumboPas encore d'évaluation
- محاضرة رقم 3 البرهانDocument38 pagesمحاضرة رقم 3 البرهانareejjooryPas encore d'évaluation
- Bronchial Asthma in Children For StudentsDocument89 pagesBronchial Asthma in Children For StudentsRasha Al MousaPas encore d'évaluation
- Bronchial Asthma (I, II &III) LecturesDocument102 pagesBronchial Asthma (I, II &III) Lecturesibnbasheer100% (5)
- History Taking Checklist.Document4 pagesHistory Taking Checklist.لو ترىPas encore d'évaluation
- Importance of Education in Bronchial Asthma TreatmDocument8 pagesImportance of Education in Bronchial Asthma TreatmRebina MoirangthemPas encore d'évaluation
- Manuel Richards - Nasal Polyps Treatment Miracle EbookDocument23 pagesManuel Richards - Nasal Polyps Treatment Miracle EbookshandoshPas encore d'évaluation
- Nursing Care PlanDocument9 pagesNursing Care PlanBishwajitMazumderPas encore d'évaluation
- Gastro Oesophageal RefluxDocument7 pagesGastro Oesophageal Refluxjustifieda13Pas encore d'évaluation
- FNCPDocument6 pagesFNCPJade Caroline OrbasePas encore d'évaluation
- Task 3 - DraftingDocument20 pagesTask 3 - Drafting30-09 STEVE JOBSPas encore d'évaluation
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Review: Ediatric NursingDocument142 pagesReview: Ediatric NursingBuRiO03Pas encore d'évaluation
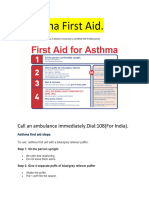
- Asthama First Aid.Document3 pagesAsthama First Aid.Manoj KumarPas encore d'évaluation
- CPD 1-CPG For The Management of Childhood AsthmaDocument43 pagesCPD 1-CPG For The Management of Childhood AsthmaizatisarefPas encore d'évaluation
- Etm 20 6 9260 PDFDocument7 pagesEtm 20 6 9260 PDFLina UkagoPas encore d'évaluation
- COPD: Epidemiology, Pathogenesis, & Pathophysiology: Wyatt E. Rousseau, MD May 11, 2006Document50 pagesCOPD: Epidemiology, Pathogenesis, & Pathophysiology: Wyatt E. Rousseau, MD May 11, 2006Mahmmoud Fuqaha100% (1)
- Allergic Rhinitis and Its Impact On Asthma (Allergy, 2008)Document153 pagesAllergic Rhinitis and Its Impact On Asthma (Allergy, 2008)incaudasemperPas encore d'évaluation
- Acute Response of Serum Leptin To Short Single Bout Exercise in Patients With Moderate AsthmaDocument8 pagesAcute Response of Serum Leptin To Short Single Bout Exercise in Patients With Moderate AsthmaOpenaccess Research paperPas encore d'évaluation
- Spray Painting and IsocyanatesDocument21 pagesSpray Painting and IsocyanatesDel MerePas encore d'évaluation
- Frankincense Essential Oil - 25 Ways To Use ItDocument2 pagesFrankincense Essential Oil - 25 Ways To Use ItTrenkc VyrsPas encore d'évaluation
- Dexamethasone (Drug Study)Document4 pagesDexamethasone (Drug Study)Franz.thenurse688871% (7)
- Case Study On AsthmaDocument21 pagesCase Study On AsthmaJerome Vergara75% (4)
- Mid Exam - General Pathology Ii - Siahs - Karim Ullah - Su-17!01!154-012Document6 pagesMid Exam - General Pathology Ii - Siahs - Karim Ullah - Su-17!01!154-012Bilal KhanPas encore d'évaluation
- Xii English CoreDocument122 pagesXii English CoreShashwat Vyas0% (2)
- Pneumonia: PathophysiologyDocument3 pagesPneumonia: PathophysiologyJanmari DavidPas encore d'évaluation
- History Taking in Clinical Practice 2023Document164 pagesHistory Taking in Clinical Practice 2023imran karimPas encore d'évaluation
- Revised Output 5Document3 pagesRevised Output 5Den AnacayPas encore d'évaluation
- Asthma BrochureDocument2 pagesAsthma BrochureRex Arisugawa100% (3)
- The Immunological Basis of The Hygiene HypothesisDocument19 pagesThe Immunological Basis of The Hygiene HypothesisRoxana Alarcón VásquezPas encore d'évaluation
- Exercise-Induced Bronchospasm (EIB) : Proposed By: Mrs. Sharry Mae G. Awayan, RN, MANDocument2 pagesExercise-Induced Bronchospasm (EIB) : Proposed By: Mrs. Sharry Mae G. Awayan, RN, MANFranz goPas encore d'évaluation
- The Age of Magical Overthinking: Notes on Modern IrrationalityD'EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityÉvaluation : 4 sur 5 étoiles4/5 (24)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisD'EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisÉvaluation : 4.5 sur 5 étoiles4.5/5 (42)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsD'EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsPas encore d'évaluation
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedD'EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedÉvaluation : 5 sur 5 étoiles5/5 (80)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsD'EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsÉvaluation : 5 sur 5 étoiles5/5 (1)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaD'EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)