Vous aimerez peut-être aussi
- Koinfeksi TB Hiv Template BaruDocument84 pagesKoinfeksi TB Hiv Template BaruAfifkurnia KurniaPas encore d'évaluation
- Yang - Gram Negative Pneumonia in The ICUDocument55 pagesYang - Gram Negative Pneumonia in The ICUAfifkurnia KurniaPas encore d'évaluation
- Welte - CAP and TB PDFDocument63 pagesWelte - CAP and TB PDFAfifkurnia KurniaPas encore d'évaluation
- Sethi - Antibiotics For AECOPDDocument52 pagesSethi - Antibiotics For AECOPDAfifkurnia KurniaPas encore d'évaluation
- Yang - Gram Negative Pneumonia in The ICUDocument55 pagesYang - Gram Negative Pneumonia in The ICUAfifkurnia KurniaPas encore d'évaluation
- Lee - Antibiotic StewardshipDocument47 pagesLee - Antibiotic StewardshipAfifkurnia KurniaPas encore d'évaluation
- Lee - Antibiotic StewardshipDocument47 pagesLee - Antibiotic StewardshipAfifkurnia KurniaPas encore d'évaluation
- Hurst - Case Presentation - Biomarkers in PracticeDocument23 pagesHurst - Case Presentation - Biomarkers in PracticeAfifkurnia KurniaPas encore d'évaluation
- 9th Asian RTI Forum Abstract BookletDocument13 pages9th Asian RTI Forum Abstract BookletAfifkurnia KurniaPas encore d'évaluation
- Cao - Emerging Trends in Resistance in AsiaDocument44 pagesCao - Emerging Trends in Resistance in AsiaAfifkurnia KurniaPas encore d'évaluation
- Disclaimer - 9th Asian RTI Forum Abstract BookletDocument13 pagesDisclaimer - 9th Asian RTI Forum Abstract BookletAfifkurnia KurniaPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Understanding and Managing Pain in Irritable Bowel Syndrome (IBS)Document4 pagesUnderstanding and Managing Pain in Irritable Bowel Syndrome (IBS)oooooPas encore d'évaluation
- A Scaled Version of The General Health Questionnaire: D. P. Goldberg and V. F. HillierDocument7 pagesA Scaled Version of The General Health Questionnaire: D. P. Goldberg and V. F. HillierKinza ChudaryPas encore d'évaluation
- Interpreting Lab Tests for Hepatitis and DiabetesDocument3 pagesInterpreting Lab Tests for Hepatitis and DiabetesShashi KumarPas encore d'évaluation
- The Logic of Immunity Deciphering An EnigmaDocument204 pagesThe Logic of Immunity Deciphering An EnigmaSatyabrataSahaPas encore d'évaluation
- Health QuizDocument6 pagesHealth QuizBrith FranklinPas encore d'évaluation
- Infection Control BasicsDocument10 pagesInfection Control BasicsAlan Amato100% (1)
- 1602126330Document65 pages1602126330AnshulAggarwal100% (1)
- Sensorineural Hearing LossDocument19 pagesSensorineural Hearing LossBenitaPas encore d'évaluation
- Smelling: Module 3 - Looking Forward: Reading Text Section C, Your HealthDocument1 pageSmelling: Module 3 - Looking Forward: Reading Text Section C, Your HealthAmalia Reyes FuentesPas encore d'évaluation
- Malaria Case AnalysisDocument1 pageMalaria Case AnalysisANGELA MARIE VILLENAPas encore d'évaluation
- Chapter # 79 - ImmunoprophylaxisDocument12 pagesChapter # 79 - Immunoprophylaxismuhammadjunaid2910Pas encore d'évaluation
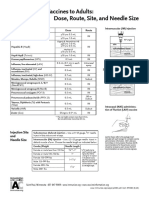
- Administering Vaccines To Adults: Dose, Route, Site, and Needle SizeDocument1 pageAdministering Vaccines To Adults: Dose, Route, Site, and Needle SizeAkashPas encore d'évaluation
- Systemic Inflammatory Response Syndrome (SIRS) : Where Did It Come From and Is It Still Relevant Today?Document7 pagesSystemic Inflammatory Response Syndrome (SIRS) : Where Did It Come From and Is It Still Relevant Today?Zulma CuevasPas encore d'évaluation
- 2012 Pall Care For Pancreas CancerDocument6 pages2012 Pall Care For Pancreas CancerFilip IonescuPas encore d'évaluation
- Virtual Conference on Organic Beef Cattle and Veterinary HomeopathyDocument4 pagesVirtual Conference on Organic Beef Cattle and Veterinary HomeopathyShubhaprada S GothePas encore d'évaluation
- Impact of Advertising Food To Pakistan Television On ChildrenDocument14 pagesImpact of Advertising Food To Pakistan Television On Childrenalim110Pas encore d'évaluation
- Hirsutism and HomoeopathyDocument9 pagesHirsutism and HomoeopathyDr. Rajneesh Kumar Sharma MD HomPas encore d'évaluation
- Hipertensi PulmonalDocument15 pagesHipertensi Pulmonaldevi efrinaPas encore d'évaluation
- Chapter 5 Prep U.odtDocument6 pagesChapter 5 Prep U.odtLivan MartellPas encore d'évaluation
- CAD plaque builds in arteries causes chest painDocument3 pagesCAD plaque builds in arteries causes chest painJoyVee Pillagara-De LeonPas encore d'évaluation
- Morphology Of The Pada Asc By Dr. Suresh Chandra MishraDocument12 pagesMorphology Of The Pada Asc By Dr. Suresh Chandra Mishraadya_tripathiPas encore d'évaluation
- Subclinical Thyroid DiseaseDocument50 pagesSubclinical Thyroid Diseaseกรคุง ภิญโญพจนารถPas encore d'évaluation
- Symptoms of Mold PoisoningDocument2 pagesSymptoms of Mold PoisoningIris Brooks100% (2)
- WBC Non Neoplastic DisordersDocument10 pagesWBC Non Neoplastic Disordersthomas palmejarPas encore d'évaluation
- Aquatic Physics: Relative DensityDocument18 pagesAquatic Physics: Relative DensitymilananandPas encore d'évaluation
- Data Interpretation For Medical Students PDFDocument905 pagesData Interpretation For Medical Students PDFMarPas encore d'évaluation
- Heart Disease in PregnancyDocument5 pagesHeart Disease in PregnancyAngeliquePas encore d'évaluation
- Tick-Borne Diseases in Turkey A Review One Health ApproachDocument12 pagesTick-Borne Diseases in Turkey A Review One Health ApproachAamir muse osmanPas encore d'évaluation
- Summary of FindingsDocument4 pagesSummary of FindingsArtemio L DumaoangPas encore d'évaluation
- Gallstones: Mitchell Conn Educational GoalsDocument8 pagesGallstones: Mitchell Conn Educational GoalsIan Evan LeePas encore d'évaluation