Vous aimerez peut-être aussi
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- 1.3b Medico-Legal Aspect of Sex CrimesDocument2 pages1.3b Medico-Legal Aspect of Sex CrimesJaybee SarmientoPas encore d'évaluation
- Contemporary Philippine Arts From The Regions: Quarter 2 - Module 9 Different Contemporary Art Techniques and PerformanceDocument25 pagesContemporary Philippine Arts From The Regions: Quarter 2 - Module 9 Different Contemporary Art Techniques and PerformanceGrace06 Labin100% (7)
- Thyroid Hormones & Anti Thyroid AgentsDocument3 pagesThyroid Hormones & Anti Thyroid AgentsJaybee SarmientoPas encore d'évaluation
- Soldier of Fortune PDFDocument208 pagesSoldier of Fortune PDFNixel SpielPas encore d'évaluation
- Immigrant Italian Stone CarversDocument56 pagesImmigrant Italian Stone Carversglis7100% (2)
- Napoleonic WargamingDocument13 pagesNapoleonic WargamingandyPas encore d'évaluation
- Stepan Formulation 926Document2 pagesStepan Formulation 926Moaz SiddigPas encore d'évaluation
- IMO Ship Waste Delivery Receipt Mepc - Circ - 645Document1 pageIMO Ship Waste Delivery Receipt Mepc - Circ - 645wisnukerPas encore d'évaluation
- ENT - Anatomy and Physiology of The Oral CavityDocument3 pagesENT - Anatomy and Physiology of The Oral CavityJaybee Sarmiento100% (2)
- Study The Effect of Postharvest Heat Treatment On Infestation Rate of Fruit Date Palm (Phoenix Dactylifera L.) Cultivars Grown in AlgeriaDocument4 pagesStudy The Effect of Postharvest Heat Treatment On Infestation Rate of Fruit Date Palm (Phoenix Dactylifera L.) Cultivars Grown in AlgeriaJournal of Nutritional Science and Healthy DietPas encore d'évaluation
- Partial Empty Sella Syndrome - A Case Report and ReviewDocument4 pagesPartial Empty Sella Syndrome - A Case Report and ReviewJaybee SarmientoPas encore d'évaluation
- For The Boards Summary of Metabolic Pathways BiochemDocument4 pagesFor The Boards Summary of Metabolic Pathways BiochemJaybee SarmientoPas encore d'évaluation
- Dr. P.Narasimha Reddy, MD Da Narayana Medical College, NelloreDocument90 pagesDr. P.Narasimha Reddy, MD Da Narayana Medical College, NelloreJaybee SarmientoPas encore d'évaluation
- Topnotch Microbiology Supertable by DR - Cocoy Calderon Jaffar Pineda Troy Soberano UPDATED NOVEMBER 2017Document16 pagesTopnotch Microbiology Supertable by DR - Cocoy Calderon Jaffar Pineda Troy Soberano UPDATED NOVEMBER 2017Jaybee Sarmiento100% (1)
- Arthropods PowerpointDocument61 pagesArthropods PowerpointJaybee SarmientoPas encore d'évaluation
- Tetracyclines, Macrolides & OthersDocument3 pagesTetracyclines, Macrolides & OthersJaybee SarmientoPas encore d'évaluation
- 1.3c EvidenceDocument1 page1.3c EvidenceJaybee SarmientoPas encore d'évaluation
- Anatomy Mock Pracs 7thDocument1 pageAnatomy Mock Pracs 7thJaybee SarmientoPas encore d'évaluation
- Highway-And-Railroad-Engineering SummaryDocument15 pagesHighway-And-Railroad-Engineering SummaryRodin James GabrilloPas encore d'évaluation
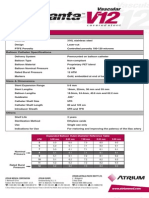
- Advanta V12 Data SheetDocument2 pagesAdvanta V12 Data SheetJuliana MiyagiPas encore d'évaluation
- Table Equivalent Schedule 40 Steel PipeDocument1 pageTable Equivalent Schedule 40 Steel PipeorisPas encore d'évaluation
- Math AA SL P 1 Marks SchemeDocument6 pagesMath AA SL P 1 Marks SchemeMrin GhoshPas encore d'évaluation
- Halfen Cast-In Channels: HTA-CE 50/30P HTA-CE 40/22PDocument92 pagesHalfen Cast-In Channels: HTA-CE 50/30P HTA-CE 40/22PTulusPas encore d'évaluation
- TreesDocument69 pagesTreesADITYA GEHLAWATPas encore d'évaluation
- Improve On-Time DeliveriesDocument24 pagesImprove On-Time DeliveriesUdayPas encore d'évaluation
- Emw 2007 FP 02093Document390 pagesEmw 2007 FP 02093boj87Pas encore d'évaluation
- Determination of Drop-Impact Resistance of Plastic BottlesDocument11 pagesDetermination of Drop-Impact Resistance of Plastic BottlesAndres BrañaPas encore d'évaluation
- Guia de CondensadoresDocument193 pagesGuia de CondensadoresPaola Segura CorreaPas encore d'évaluation
- Fully Automatic Coffee Machine - Slimissimo - IB - SCOTT UK - 2019Document20 pagesFully Automatic Coffee Machine - Slimissimo - IB - SCOTT UK - 2019lazareviciPas encore d'évaluation
- Fundamentals of Pain Medicine: Jianguo Cheng Richard W. RosenquistDocument346 pagesFundamentals of Pain Medicine: Jianguo Cheng Richard W. RosenquistMayPas encore d'évaluation
- G1CDocument12 pagesG1CKhriz Ann C ÜPas encore d'évaluation
- Assignment 2 Mat435Document2 pagesAssignment 2 Mat435Arsene LupinPas encore d'évaluation
- Elements of Romanticism in The Poetry of W. B. Yeats: Romantic InfluencesDocument8 pagesElements of Romanticism in The Poetry of W. B. Yeats: Romantic InfluencesSadman Shaid SaadPas encore d'évaluation
- C.Abdul Hakeem College of Engineering and Technology, Melvisharam Department of Aeronautical Engineering Academic Year 2020-2021 (ODD)Document1 pageC.Abdul Hakeem College of Engineering and Technology, Melvisharam Department of Aeronautical Engineering Academic Year 2020-2021 (ODD)shabeerPas encore d'évaluation
- 3rd Quarter Exam (Statistics)Document4 pages3rd Quarter Exam (Statistics)JERALD MONJUANPas encore d'évaluation
- Industrial Artificial Intelligence For Industry 4.0-Based Manufacturing SystemsDocument5 pagesIndustrial Artificial Intelligence For Industry 4.0-Based Manufacturing SystemsMuhammad HaziqPas encore d'évaluation
- 12/1/2014 Powder MetallurgyDocument29 pages12/1/2014 Powder Metallurgysofyan sam0% (2)
- Amnaya Sutra (English)Document458 pagesAmnaya Sutra (English)Assam Bhakti SagarPas encore d'évaluation
- Electricity NotesDocument35 pagesElectricity Notesapi-277818647Pas encore d'évaluation
- A Year On A FarmDocument368 pagesA Year On A FarmvehapkolaPas encore d'évaluation
- Socialized HousingDocument48 pagesSocialized HousingJessieReiVicedoPas encore d'évaluation