Vous aimerez peut-être aussi
- NPS MedicineWise Thyroid Testing Algorithm v3Document1 pageNPS MedicineWise Thyroid Testing Algorithm v3Mikhael JHPas encore d'évaluation
- Thyroid Disorders Testing AlgorithmDocument1 pageThyroid Disorders Testing AlgorithmMuhamad SuriansyahPas encore d'évaluation
- Thyroid Disorders Testing AlgorithmDocument1 pageThyroid Disorders Testing AlgorithmRezi HelperPas encore d'évaluation
- Pa Tho PhysiologyDocument2 pagesPa Tho PhysiologyArnel Luces BeatoPas encore d'évaluation
- Pemeriksaan Laboratorium Hormon Tiroid: Oleh: Dr. Diah Hermayanti, SPPKDocument16 pagesPemeriksaan Laboratorium Hormon Tiroid: Oleh: Dr. Diah Hermayanti, SPPKZulfan RifqiawanPas encore d'évaluation
- Low Free T4 Normal Free T4 High Free T4Document3 pagesLow Free T4 Normal Free T4 High Free T4Joseph De JoyaPas encore d'évaluation
- Assessment of Thyroid FunctionDocument7 pagesAssessment of Thyroid FunctionDewi Paramita YuniarahmiPas encore d'évaluation
- TFT Interpretation of Difficult CasesDocument51 pagesTFT Interpretation of Difficult CasesAditya GautamPas encore d'évaluation
- 803 FullDocument9 pages803 FullSuvPas encore d'évaluation
- Thyroid Tests and ResultsDocument9 pagesThyroid Tests and ResultsKristel BelgicaPas encore d'évaluation
- Approach To A Low TSH Level - Patience Is A Virtue PDFDocument10 pagesApproach To A Low TSH Level - Patience Is A Virtue PDFDonovan KylePas encore d'évaluation
- Thyroid Disorders Testing AlgorithmDocument1 pageThyroid Disorders Testing AlgorithmkatPas encore d'évaluation
- Endocrinology Part 2Document4 pagesEndocrinology Part 2Alondra SagarioPas encore d'évaluation
- Thyroid Function Test 12-2-09Document69 pagesThyroid Function Test 12-2-09Romaysaamohamed AlyPas encore d'évaluation
- Thyroid Function Ordering AlgorithmDocument1 pageThyroid Function Ordering AlgorithmMVKDSP RaoPas encore d'évaluation
- Thyroid Disease (Chan)Document29 pagesThyroid Disease (Chan)Sidiq AboobakerPas encore d'évaluation
- Thyroid Function Tests (TFT'S) : Roll No 04Document22 pagesThyroid Function Tests (TFT'S) : Roll No 04Ajay YAPas encore d'évaluation
- Clinical Practice Guidelines For Hypothyroidism in Adults: AACE and ATA 2012Document63 pagesClinical Practice Guidelines For Hypothyroidism in Adults: AACE and ATA 2012Nur Rakhma AkmaliaPas encore d'évaluation
- TSH Reagent Kit: B7P480 G71292R02Document6 pagesTSH Reagent Kit: B7P480 G71292R02Галина МиловановаPas encore d'évaluation
- Laboratory Diagnostics of (Selected) Endocrine DisordersDocument48 pagesLaboratory Diagnostics of (Selected) Endocrine DisordersPaulina PaskeviciutePas encore d'évaluation
- Thyroid Function Test: The "Hidden" Health ProblemDocument34 pagesThyroid Function Test: The "Hidden" Health Problemvjanand07100% (1)
- Thyroid Function Tests: Drneha Mahajan MD PathologyDocument71 pagesThyroid Function Tests: Drneha Mahajan MD PathologyMukesh Kumar ChaudharyPas encore d'évaluation
- TRH Stimulation TestDocument3 pagesTRH Stimulation TestsakuraleeshaoranPas encore d'évaluation
- Endocrinology - 02 (3) - Thyroid Disorders (Courses in Therapeutics and Disease State Management)Document17 pagesEndocrinology - 02 (3) - Thyroid Disorders (Courses in Therapeutics and Disease State Management)Ali AlyahawiPas encore d'évaluation
- Hypothalamus Pituitary Thyroid AxisDocument15 pagesHypothalamus Pituitary Thyroid AxisEdmari Joy Pojas MontilPas encore d'évaluation
- Thyroid Talk-FMD RdsDocument58 pagesThyroid Talk-FMD RdsSriman YarrarapuPas encore d'évaluation
- Thyroid Function TestsDocument29 pagesThyroid Function TestsAkwesaPas encore d'évaluation
- Guidelines For The Management of Thyrotoxicosis (May 2014) PDFDocument30 pagesGuidelines For The Management of Thyrotoxicosis (May 2014) PDFFarman JaaferPas encore d'évaluation
- Algoritma Hipo Dan HipertiroidDocument1 pageAlgoritma Hipo Dan HipertiroidDamn YeahPas encore d'évaluation
- HYPERTHYROIDISMDocument1 pageHYPERTHYROIDISMAmber BlodduweddPas encore d'évaluation
- Thyroid Function Tests and Goitre SV 24-4-21Document51 pagesThyroid Function Tests and Goitre SV 24-4-21Lal KhanPas encore d'évaluation
- Hpa HptaxeschartDocument2 pagesHpa Hptaxeschartdikadika_tansPas encore d'évaluation
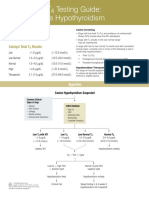
- Catalyst One Total t4 Testing Guide en PDFDocument2 pagesCatalyst One Total t4 Testing Guide en PDFИрина ВладимироваPas encore d'évaluation
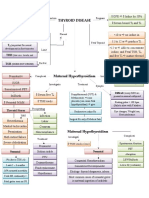
- Thyroid DiseaseDocument1 pageThyroid DiseaseZiyadPas encore d'évaluation
- RTH 1Document3 pagesRTH 1Ei DrakorPas encore d'évaluation
- Kate PlanchetDocument29 pagesKate Planchetsundance127Pas encore d'évaluation
- Thyroid Function TestDocument34 pagesThyroid Function TestAishaPas encore d'évaluation
- Testing Strategies For Thyroid EvaluationDocument18 pagesTesting Strategies For Thyroid EvaluationcoassukoyPas encore d'évaluation
- Disorders of Thyroid Gland - S.D Osuntoye-1Document32 pagesDisorders of Thyroid Gland - S.D Osuntoye-1IiiPas encore d'évaluation
- Pharmacology Finals Lecture Thyroid DisordersDocument11 pagesPharmacology Finals Lecture Thyroid DisordersJuliann100% (1)
- FunctionTests BrochureDocument2 pagesFunctionTests Brochurejonalyntonato09Pas encore d'évaluation
- Hypothyroidism Diagnosis FlowchartDocument1 pageHypothyroidism Diagnosis FlowchartKim Yang ChongPas encore d'évaluation
- Total t4 Testing Guide Cat UnifiedDocument2 pagesTotal t4 Testing Guide Cat UnifiedAndreea MayaPas encore d'évaluation
- Thyroid Disorders: Disease Description Thyroid Panel Results Diagnostic/ Specific Tests For DiagnosisDocument2 pagesThyroid Disorders: Disease Description Thyroid Panel Results Diagnostic/ Specific Tests For DiagnosisNoreen B. BañagadoPas encore d'évaluation
- TRH Stimulation Test: Differential Diagnosis UseDocument2 pagesTRH Stimulation Test: Differential Diagnosis UseBogdan TomaPas encore d'évaluation
- (Health) Thyroid Functions TestsDocument4 pages(Health) Thyroid Functions Testsmahendra3107Pas encore d'évaluation
- Thyroid Function TestsDocument15 pagesThyroid Function TestsJoseline AlicePas encore d'évaluation
- Chapter 47Document19 pagesChapter 47Javier Burgos CárdenasPas encore d'évaluation
- EAU Pocket On Sexual and Reproductive Health 2023Document65 pagesEAU Pocket On Sexual and Reproductive Health 2023Alexander Joel Guzmán CórdovaPas encore d'évaluation
- Hypothalamic Pitutary Axis and Thyroid Hormone SynthesisDocument5 pagesHypothalamic Pitutary Axis and Thyroid Hormone Synthesis78 shivangi mauryaPas encore d'évaluation
- Thyroid Function Test (TFT)Document16 pagesThyroid Function Test (TFT)PAPUN KUMAR ROUTPas encore d'évaluation
- 10 16 Thyroid Function NitinDocument7 pages10 16 Thyroid Function NitinStrawberry ShortcakePas encore d'évaluation
- Interpretasi TiroidDocument6 pagesInterpretasi TiroidSagita MuliaPas encore d'évaluation
- Ok Bab 20 Reproduction and Thyroid (Ky)Document22 pagesOk Bab 20 Reproduction and Thyroid (Ky)rista silvanaPas encore d'évaluation
- 6e - Thyroid Dysfunction in Pregnancy A Literature Review (Perbaiki Dafpus)Document5 pages6e - Thyroid Dysfunction in Pregnancy A Literature Review (Perbaiki Dafpus)KESEBELASAN RESOG 2023Pas encore d'évaluation
- T4 Reactiv ChemiluminiscentaDocument5 pagesT4 Reactiv ChemiluminiscentaLidia NarbPas encore d'évaluation
- Disorders of The Thyroid: OutlineDocument9 pagesDisorders of The Thyroid: OutlineMelissa-Andreea Ardeleanu Carvajal OsorioPas encore d'évaluation
- Thyroiddisease 190216062020Document42 pagesThyroiddisease 190216062020Manikandan Vp100% (1)
- Managing Thyroid Disease in General PracticeDocument6 pagesManaging Thyroid Disease in General PracticeEmir SaricPas encore d'évaluation
- DS POC Nasopharyngeal-collection-For-Veritor IM enDocument1 pageDS POC Nasopharyngeal-collection-For-Veritor IM endjebrut100% (1)
- ILKI - UndanganDocument3 pagesILKI - UndangandjebrutPas encore d'évaluation
- Pme BBLK 2019Document4 pagesPme BBLK 2019djebrutPas encore d'évaluation
- E 411 Assay Summary Aug 2023 Rev3 - H I LDocument1 pageE 411 Assay Summary Aug 2023 Rev3 - H I LdjebrutPas encore d'évaluation
- AlbuminDocument1 pageAlbumindjebrutPas encore d'évaluation
- OriginalarticleDocument5 pagesOriginalarticledjebrutPas encore d'évaluation
- Kriteria Remisi AmlDocument6 pagesKriteria Remisi AmldjebrutPas encore d'évaluation
- Hem - Lab 4 Retic - 09Document9 pagesHem - Lab 4 Retic - 09djebrutPas encore d'évaluation
- Classic Methods Revisited: Widal Agglutination Test 100 Years Later: Still Plagued by ControversyDocument6 pagesClassic Methods Revisited: Widal Agglutination Test 100 Years Later: Still Plagued by ControversydjebrutPas encore d'évaluation
- Laboratory Utilization in The Emergency Department - Are The Requested Tests Patient-Oriented?Document3 pagesLaboratory Utilization in The Emergency Department - Are The Requested Tests Patient-Oriented?djebrutPas encore d'évaluation
- 734 FullDocument7 pages734 FulldjebrutPas encore d'évaluation
- 77 FullDocument7 pages77 FulldjebrutPas encore d'évaluation
- 0812 in Vitro Blood Gas Analyzers GuideDocument9 pages0812 in Vitro Blood Gas Analyzers GuidedjebrutPas encore d'évaluation
- 249 FullDocument4 pages249 FulldjebrutPas encore d'évaluation
- Different Diagnostic Procedure of Typhoid Fever ADocument8 pagesDifferent Diagnostic Procedure of Typhoid Fever AdjebrutPas encore d'évaluation
- Conjugated Hyperbilirubinemia:: Screening and Treatment in Older Infants and ChildrenDocument11 pagesConjugated Hyperbilirubinemia:: Screening and Treatment in Older Infants and ChildrendjebrutPas encore d'évaluation
- PriceList-APAR GMP-TerbaruDocument35 pagesPriceList-APAR GMP-TerbarudjebrutPas encore d'évaluation
- Leaflet QC SeminarDocument2 pagesLeaflet QC SeminardjebrutPas encore d'évaluation
- External Examination at AutopsyDocument87 pagesExternal Examination at AutopsyDr. Ashish JawarkarPas encore d'évaluation
- Antipsychotics Pharm 3 Year 2Document19 pagesAntipsychotics Pharm 3 Year 2Dua'a Al-HamdanPas encore d'évaluation
- Pereneal CareDocument2 pagesPereneal CareindumathiPas encore d'évaluation
- ACT Guide-Final PDFDocument25 pagesACT Guide-Final PDFedw68Pas encore d'évaluation
- Grass Jelly On Glycemic ControlDocument11 pagesGrass Jelly On Glycemic ControlAnanta ArioPas encore d'évaluation
- MSQH 5th Edition Standard 08 - Emergency Services-Jan 2017Document28 pagesMSQH 5th Edition Standard 08 - Emergency Services-Jan 2017Siti HusniPas encore d'évaluation
- How To Make Ginger CandyDocument4 pagesHow To Make Ginger CandyJun Jihad BarrogaPas encore d'évaluation
- StahleDocument12 pagesStahlekhaledazima0% (2)
- Ankle Foot InjuriesDocument85 pagesAnkle Foot InjuriesDoc DelowerPas encore d'évaluation
- Name: Angel May P. Agot Listing and Categorizing of Health Problems Address: List of Problems in Our CommunityDocument4 pagesName: Angel May P. Agot Listing and Categorizing of Health Problems Address: List of Problems in Our CommunityAngel MayPas encore d'évaluation
- Effectofcorestabilityexerciseonposturalstabilityinchildrenwith DownsyndromeDocument11 pagesEffectofcorestabilityexerciseonposturalstabilityinchildrenwith Downsyndrome8 nocturnalPas encore d'évaluation
- Start Los AngelesDocument10 pagesStart Los AngelesIGDPas encore d'évaluation
- Ich GCP: HistoryDocument57 pagesIch GCP: HistoryChandrashekhar Singh100% (1)
- Geriatric AssessmentDocument27 pagesGeriatric AssessmentNeil Philip MaturanPas encore d'évaluation
- Aditya MotwaneDocument3 pagesAditya Motwaneapi-257938623Pas encore d'évaluation
- HPP Dan ShockDocument54 pagesHPP Dan ShockAntok JegauPas encore d'évaluation
- Global Epidemiology of Oral and Oropharyngeal CancerDocument8 pagesGlobal Epidemiology of Oral and Oropharyngeal CancerArpit JainPas encore d'évaluation
- DPA Ally Fall 08Document8 pagesDPA Ally Fall 08webmaster@drugpolicy.orgPas encore d'évaluation
- HypochondriasisDocument2 pagesHypochondriasisThe LullabyPas encore d'évaluation
- Part 6 Anesthesiology: Anesthesiology and Its DevelopmentDocument24 pagesPart 6 Anesthesiology: Anesthesiology and Its DevelopmentburhaninhoPas encore d'évaluation
- Discovery: Advanced Point-of-Care Bone Health AssessmentDocument12 pagesDiscovery: Advanced Point-of-Care Bone Health AssessmentNasr Eldin AlyPas encore d'évaluation
- Genital HerpesDocument2 pagesGenital HerpesWisnu WardanaPas encore d'évaluation
- Of Thyroid and Antithyroid Drugs - Part IIDocument16 pagesOf Thyroid and Antithyroid Drugs - Part IIVikas Viki100% (1)
- Shamanism and Altered States of ConsciousnessDocument15 pagesShamanism and Altered States of Consciousnessyodoid100% (2)
- A Veteran's Re-Adjustment and Extensional Methods by Alfred Korzybski (1945)Document12 pagesA Veteran's Re-Adjustment and Extensional Methods by Alfred Korzybski (1945)Anonymous yu09qxYCMPas encore d'évaluation
- Safety at Gasoline StationDocument7 pagesSafety at Gasoline StationBudiman -Pas encore d'évaluation
- FMC Network Provider List - Dhaen2 Plan: Area Providers Name Provide RS Emirate SDocument39 pagesFMC Network Provider List - Dhaen2 Plan: Area Providers Name Provide RS Emirate SMuhammad SiddiuqiPas encore d'évaluation
- Pacemakers Cardiac External Invasive Electrodes TransvenousDocument6 pagesPacemakers Cardiac External Invasive Electrodes TransvenousEduardoPas encore d'évaluation
- Medical Malpractice (DR Jarcia Vs People)Document8 pagesMedical Malpractice (DR Jarcia Vs People)Francesco Celestial BritanicoPas encore d'évaluation