Vous aimerez peut-être aussi
- A Strategic Guide to Continuing Professional Development for Health and Care Professionals: The TRAMm ModelD'EverandA Strategic Guide to Continuing Professional Development for Health and Care Professionals: The TRAMm ModelPas encore d'évaluation
- Textbook of Urgent Care Management: Chapter 34, Engaging Accountable Care Organizations in Urgent Care CentersD'EverandTextbook of Urgent Care Management: Chapter 34, Engaging Accountable Care Organizations in Urgent Care CentersPas encore d'évaluation
- Year One of Practice Transition: The Necessary Guide to SuccessD'EverandYear One of Practice Transition: The Necessary Guide to SuccessJason E. PopePas encore d'évaluation
- Critique of The Effect of Complementary Music Therapy On The Patient's Postoperative State Anxiety, Pain Control, and Environmental Noise SatisfactionDocument12 pagesCritique of The Effect of Complementary Music Therapy On The Patient's Postoperative State Anxiety, Pain Control, and Environmental Noise SatisfactionAndrew AdlaonPas encore d'évaluation
- Sonu Scaria Literature ReviewDocument13 pagesSonu Scaria Literature ReviewAnonymous aUrycuWgyPas encore d'évaluation
- JBI Checklist For RCTs Archive 2020Document11 pagesJBI Checklist For RCTs Archive 2020Abigael StephanniePas encore d'évaluation
- Comprehensive Nursing Assessment ToolDocument7 pagesComprehensive Nursing Assessment ToolRamesh KandagatlaPas encore d'évaluation
- OT Models PratciceDocument30 pagesOT Models PratciceWalaa Eldesoukey100% (1)
- Whatis Critical AppraisalDocument8 pagesWhatis Critical Appraisalapi-3861522Pas encore d'évaluation
- What Is A PICO QuestionDocument3 pagesWhat Is A PICO QuestionBoid Gerodias100% (2)
- Ebook Nursing CollectionDocument88 pagesEbook Nursing CollectionTiffany MartinezPas encore d'évaluation
- Integrative Literature AutosavedDocument21 pagesIntegrative Literature Autosavedapi-486981186Pas encore d'évaluation
- This Study Resource Was: Student Name: Madeline Hammett HAMMD1901Document5 pagesThis Study Resource Was: Student Name: Madeline Hammett HAMMD1901Ambika Suwal100% (1)
- Module 3 Reflective Essay GuidanceDocument10 pagesModule 3 Reflective Essay GuidanceKainatPas encore d'évaluation
- NS 622 AssignmentDocument16 pagesNS 622 AssignmentGareth McKnightPas encore d'évaluation
- Interprofessional Team Reduces Fall RatesDocument11 pagesInterprofessional Team Reduces Fall RatesAbdulWakhidPas encore d'évaluation
- Writing Goals and Objectives: An Integral Part of An Online CourseDocument25 pagesWriting Goals and Objectives: An Integral Part of An Online CourseLeslie Butlig JudayaPas encore d'évaluation
- Introduction to Nursing Research Part 1: Significance and MethodologyDocument22 pagesIntroduction to Nursing Research Part 1: Significance and MethodologyCiedelle Honey Lou DimaligPas encore d'évaluation
- Gibbs Using Gibbs Reflective CycleDocument4 pagesGibbs Using Gibbs Reflective CycleMuhammad Ridwan100% (1)
- Physician Burnout The Root of The Problem and The Path To SolutionsDocument52 pagesPhysician Burnout The Root of The Problem and The Path To SolutionstjelongPas encore d'évaluation
- Project Implementation SimulationDocument10 pagesProject Implementation Simulationsyeda maryemPas encore d'évaluation
- Marketing Mix - The 4 P's of Marketing ExplainedDocument6 pagesMarketing Mix - The 4 P's of Marketing ExplainedDeepak Kalonia JangraPas encore d'évaluation
- Driscoll Model Reflection: NBNS 3603 Reflective Thinking and WritingDocument15 pagesDriscoll Model Reflection: NBNS 3603 Reflective Thinking and WritingAria Sekan100% (3)
- Recent Global Epidemiology in StrokeDocument73 pagesRecent Global Epidemiology in StrokeratuhamimPas encore d'évaluation
- APTA Professionalism Core Values Self AssessmentDocument11 pagesAPTA Professionalism Core Values Self AssessmentJPPas encore d'évaluation
- Code Blue EmergenciesDocument17 pagesCode Blue EmergenciesEstherThompsonPas encore d'évaluation
- Clinical Reasoning Instructor ResourcesDocument17 pagesClinical Reasoning Instructor ResourcesMajid Jafarzadeh100% (1)
- PRISMA Extension For Scoping Reviews PRISMA SCRDocument19 pagesPRISMA Extension For Scoping Reviews PRISMA SCRJhon OrtizPas encore d'évaluation
- Test Bank For Foundations of Clinical Research Applications To Evidence Based Practice 4th Edition Leslie G PortneyDocument4 pagesTest Bank For Foundations of Clinical Research Applications To Evidence Based Practice 4th Edition Leslie G Portneymarisgemma0j3vPas encore d'évaluation
- Jadad Scale PDFDocument12 pagesJadad Scale PDFEnaik100% (1)
- Activity For Dementia PTDocument18 pagesActivity For Dementia PTclyde i amPas encore d'évaluation
- 4.73 (FCM) EBM - Critical Appraisal On Therapy and PreventionDocument6 pages4.73 (FCM) EBM - Critical Appraisal On Therapy and PreventionEver Mary Joy EscaleraPas encore d'évaluation
- Normal Growth Patterns in Infants and Prepubertal ChildrenDocument15 pagesNormal Growth Patterns in Infants and Prepubertal Childrenedu2029Pas encore d'évaluation
- Critical Appraisal EssayDocument13 pagesCritical Appraisal EssayCaren Chan67% (3)
- Running Head: Integrative Literature Review 1Document22 pagesRunning Head: Integrative Literature Review 1api-456581702Pas encore d'évaluation
- Nursing Theory PaperDocument10 pagesNursing Theory Paperapi-312364579Pas encore d'évaluation
- Self-Medication Practices Among Health S PDFDocument7 pagesSelf-Medication Practices Among Health S PDFSyed Shabbir HaiderPas encore d'évaluation
- Article Critical AppraisalDocument8 pagesArticle Critical AppraisalagdroubiPas encore d'évaluation
- Cervicovestibular Rehabilitation in Sport-Related Concussion - A Randomised Controlled TrialDocument7 pagesCervicovestibular Rehabilitation in Sport-Related Concussion - A Randomised Controlled TrialhilmikamelPas encore d'évaluation
- PDSA - Example - Ensuring Dental Charts Are CompletedDocument5 pagesPDSA - Example - Ensuring Dental Charts Are CompletedNinoslav MladenovicPas encore d'évaluation
- Sample Assignment of Nursing LeadershipDocument5 pagesSample Assignment of Nursing LeadershipPrasiddha Parajuli100% (1)
- Decision MakingDocument9 pagesDecision MakingTalhaFarrukhPas encore d'évaluation
- Debriefing With The OPT Model of Clinical ReasoningDocument16 pagesDebriefing With The OPT Model of Clinical ReasoningSri JamilahPas encore d'évaluation
- Essay - Role of PT in SportsDocument2 pagesEssay - Role of PT in SportsAlexander ScottPas encore d'évaluation
- Lecture 1-Introduction To Research & Research Methodology - PPTX Lecture 1Document21 pagesLecture 1-Introduction To Research & Research Methodology - PPTX Lecture 1Bahauddin BalochPas encore d'évaluation
- Nursing Philosophy QepDocument5 pagesNursing Philosophy Qepapi-534072530Pas encore d'évaluation
- 2015 SurveyDocument302 pages2015 SurveyJohn SmithPas encore d'évaluation
- Evidence-Based Practice Fact SheetDocument3 pagesEvidence-Based Practice Fact Sheetmohamedwhatever100% (2)
- Missed Nursing Care Qualitative-CritiqueDocument7 pagesMissed Nursing Care Qualitative-Critiquefocus16hoursgmailcom100% (1)
- Critical Pathways As A Strategy For Improving CareDocument8 pagesCritical Pathways As A Strategy For Improving CaredranandrtPas encore d'évaluation
- Rabideau Kitchen Eval AjotDocument8 pagesRabideau Kitchen Eval Ajotapi-291380671Pas encore d'évaluation
- A Successful Way For Performing Nutritional Nursing Assessment in Older Patients.Document10 pagesA Successful Way For Performing Nutritional Nursing Assessment in Older Patients.NurseSmall81Pas encore d'évaluation
- Clinical Decision Making of Nurses Working in Hospital SettingsDocument10 pagesClinical Decision Making of Nurses Working in Hospital Settingsedy harahapPas encore d'évaluation
- Johns Model of Structured ReflectionDocument1 pageJohns Model of Structured ReflectionLeeynesh Sooriyapiragasam100% (4)
- Teaching and Learning Essay Sample On MoodleDocument20 pagesTeaching and Learning Essay Sample On MoodleMuhammad Faraz Hasan100% (1)
- The Operating Department Practitioner Nursing EssayDocument5 pagesThe Operating Department Practitioner Nursing EssayNerisPas encore d'évaluation
- Assignment 2 Critical Analysis of ResearchDocument8 pagesAssignment 2 Critical Analysis of Researchapi-357644683Pas encore d'évaluation
- Written Assignment 1 HSNS171 Fundamentals of Nursing Practice 1 Word Count: 973Document7 pagesWritten Assignment 1 HSNS171 Fundamentals of Nursing Practice 1 Word Count: 973Sophie Anderson0% (1)
- Clinical ReasoningDocument4 pagesClinical Reasoningapi-351971578Pas encore d'évaluation
- Fisher (2013) Occupation-Centred Occupation-Based Occupation-FocusedDocument12 pagesFisher (2013) Occupation-Centred Occupation-Based Occupation-FocusedElianaMicaela100% (1)
- Refreactory GERDDocument50 pagesRefreactory GERDT.A.BPas encore d'évaluation
- What Are The Disadvantages of Sliding-Scale Insulin?: BriefreportDocument3 pagesWhat Are The Disadvantages of Sliding-Scale Insulin?: BriefreportT.A.BPas encore d'évaluation
- Case ReportDocument16 pagesCase ReportT.A.BPas encore d'évaluation
- Pembacaan Jurnal 21-4-15Document5 pagesPembacaan Jurnal 21-4-15T.A.BPas encore d'évaluation
- Package Office - National ChoicesDocument2 pagesPackage Office - National ChoicesT.A.BPas encore d'évaluation
- What Happens in A 5-Year Follow-Up of Benign Thyroid NodulesDocument4 pagesWhat Happens in A 5-Year Follow-Up of Benign Thyroid NodulesT.A.BPas encore d'évaluation
- 12.national Office ChoicesDocument1 page12.national Office ChoicesT.A.BPas encore d'évaluation
- Journal Reading Tiara 31-1-2017Document4 pagesJournal Reading Tiara 31-1-2017T.A.BPas encore d'évaluation
- Critical Appraisal #2 (Descriptive)Document13 pagesCritical Appraisal #2 (Descriptive)T.A.BPas encore d'évaluation
- Thyroid Disorders: Causes, Symptoms and TreatmentDocument39 pagesThyroid Disorders: Causes, Symptoms and TreatmentT.A.BPas encore d'évaluation
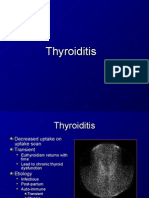
- Tugas ThyroiditisDocument9 pagesTugas ThyroiditisT.A.BPas encore d'évaluation
- Disorders of The Parathyroid GlandsDocument47 pagesDisorders of The Parathyroid GlandsTangTingPas encore d'évaluation
- Critical Appraisal PrognosisDocument4 pagesCritical Appraisal Prognosis568563Pas encore d'évaluation
- Hepatorenal SyndromeDocument2 pagesHepatorenal SyndromeT.A.BPas encore d'évaluation
- Reversible Myelopathy in A 34-Year-Old Man With Vitamin B DeficiencyDocument4 pagesReversible Myelopathy in A 34-Year-Old Man With Vitamin B DeficiencyT.A.BPas encore d'évaluation
- Alkoholic PolineuropatiDocument7 pagesAlkoholic PolineuropatiT.A.BPas encore d'évaluation
- From Solvay Magazine - 48 - Dec 2011 PDFDocument36 pagesFrom Solvay Magazine - 48 - Dec 2011 PDFchb2Pas encore d'évaluation
- Application for Pre-Hispanic Literature ActivityDocument1 pageApplication for Pre-Hispanic Literature ActivityQueenie Gonzales-AguloPas encore d'évaluation
- Cultural Humility Framework for Anti-Oppressive ArchivesDocument23 pagesCultural Humility Framework for Anti-Oppressive ArchivesVikram KalekaPas encore d'évaluation
- The What Why and How of Culturally Responsive Teaching International Mandates Challenges and OpportunitiesDocument18 pagesThe What Why and How of Culturally Responsive Teaching International Mandates Challenges and Opportunitiesapi-696560926Pas encore d'évaluation
- 2010 11catalogDocument313 pages2010 11catalogJustin PennPas encore d'évaluation
- Frei Universitat PDFDocument167 pagesFrei Universitat PDFalnaturamilkaPas encore d'évaluation
- Syllabus-Combined-Ad-No 7-2021Document7 pagesSyllabus-Combined-Ad-No 7-2021ZakirUllahPas encore d'évaluation
- Effects of Peer Pressure on Academic Performance (40Document6 pagesEffects of Peer Pressure on Academic Performance (40MaynardMiranoPas encore d'évaluation
- Researcher Development Framework RDF Planner Overview Vitae 2012Document2 pagesResearcher Development Framework RDF Planner Overview Vitae 2012Daniel GiesPas encore d'évaluation
- Goals and Syllabus: Dewanti Dian Apriliani Efi Rokhayanti Novida Fatma Dewita Priskila Shendy HartantiDocument30 pagesGoals and Syllabus: Dewanti Dian Apriliani Efi Rokhayanti Novida Fatma Dewita Priskila Shendy HartantiPriskila Shendy HartantiPas encore d'évaluation
- 1 GEN ED PRE BOARD Rabies Comes From Dog and Other BitesDocument12 pages1 GEN ED PRE BOARD Rabies Comes From Dog and Other BitesJammie Aure EsguerraPas encore d'évaluation
- 2016 CBD Application FormDocument2 pages2016 CBD Application FormAlina IliseiPas encore d'évaluation
- Cognitive and Metacognitive ProcessesDocument45 pagesCognitive and Metacognitive ProcessesjhenPas encore d'évaluation
- Leadership and Teamwork DefinedDocument22 pagesLeadership and Teamwork DefinedAyu AzlinaPas encore d'évaluation
- Your World 2022 23 Teacher Tool KitDocument4 pagesYour World 2022 23 Teacher Tool KitNICE InternationalPas encore d'évaluation
- GEC 8 Packet 1Document47 pagesGEC 8 Packet 1Jean MojadoPas encore d'évaluation
- English Teaching ProfessionalDocument64 pagesEnglish Teaching ProfessionalDanielle Soares100% (2)
- Sepep Self ReflectionDocument6 pagesSepep Self Reflectionapi-464088459Pas encore d'évaluation
- History of Philippine Cinema Research Paper TopicsDocument4 pagesHistory of Philippine Cinema Research Paper Topicsfvg2xg5rPas encore d'évaluation
- Bsbsus201 R1Document4 pagesBsbsus201 R1sanam shresthaPas encore d'évaluation
- Media LiteracyDocument16 pagesMedia LiteracyRLM100% (2)
- Resume of Sahed AhamedDocument2 pagesResume of Sahed AhamedSahed AhamedPas encore d'évaluation
- Problems On Trains - Aptitude Questions and AnswersDocument6 pagesProblems On Trains - Aptitude Questions and AnswersMuhammadNaveedPas encore d'évaluation
- Agreeing and Disagreeing WorksheetDocument3 pagesAgreeing and Disagreeing WorksheetАнастасия Сизион75% (4)
- Grade 6 Food Preservation Weekly LessonDocument67 pagesGrade 6 Food Preservation Weekly Lessonchona redillasPas encore d'évaluation
- Experiential Learning for Leadership Development Approaches, Best Practices and Case Studies-2010年Document38 pagesExperiential Learning for Leadership Development Approaches, Best Practices and Case Studies-2010年Zhijiang DouPas encore d'évaluation
- MTO Drivers Handbook For Ontario, CanadaDocument145 pagesMTO Drivers Handbook For Ontario, CanadaJo PantulaPas encore d'évaluation
- Resume 1Document1 pageResume 1api-444979830Pas encore d'évaluation
- Architecture and Design Institute Project ReportDocument103 pagesArchitecture and Design Institute Project ReportAbi Kannan100% (1)
- Benchmarks From The Talent Development Capability Model 2023 q2 With SegmentsDocument10 pagesBenchmarks From The Talent Development Capability Model 2023 q2 With Segmentspearl.yeo.atPas encore d'évaluation