Vous aimerez peut-être aussi
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Planar MetalsDocument11 pagesPlanar MetalsSilvano Prado0% (1)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Proposed OS&E Requirement - Measuring Ozone DosageDocument3 pagesProposed OS&E Requirement - Measuring Ozone DosageProteina QuitinasePas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Reading TOEFLDocument13 pagesReading TOEFLwelnitesiPas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Ets InternacionalDocument72 pagesEts InternacionalRicardo MarquesPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- 2023 Microalgae Application To Bone Repairing Process - A ReviewDocument19 pages2023 Microalgae Application To Bone Repairing Process - A ReviewvirgiparedesPas encore d'évaluation
- PAMG-PA3 5052 Aluminum Honeycomb: DescriptionDocument2 pagesPAMG-PA3 5052 Aluminum Honeycomb: Descriptionsahiljain_146Pas encore d'évaluation
- Hot Work PermitDocument2 pagesHot Work PermitRex UrbiztondoPas encore d'évaluation
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Heat Transfer To Fluids With Phase ChangeDocument9 pagesHeat Transfer To Fluids With Phase Changepraveen4ubvsPas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- ASTM Method D5134-92Document1 pageASTM Method D5134-92Sylab InstrumentsPas encore d'évaluation
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Nitrogen, Total, TNT, 0 To 25.0, Persulfate Digestion Method 10071Document9 pagesNitrogen, Total, TNT, 0 To 25.0, Persulfate Digestion Method 10071Dwiyana YogasariPas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
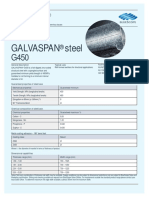
- Galvaspan G450Document2 pagesGalvaspan G450khurshedlakhoPas encore d'évaluation
- BR Int LD Id Inspiration 55-70plusDocument11 pagesBR Int LD Id Inspiration 55-70plustarkett tPas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Stepan Pol Ps 2352Document2 pagesStepan Pol Ps 2352A MahmoodPas encore d'évaluation
- Spe 180853 MSDocument18 pagesSpe 180853 MSkerron_rekhaPas encore d'évaluation
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Mass Spectral Databases For LC-MS - and GC-MS-based Metabolomics PDFDocument13 pagesMass Spectral Databases For LC-MS - and GC-MS-based Metabolomics PDFciborg1978Pas encore d'évaluation
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Tugas 1 PPADocument29 pagesTugas 1 PPAlulalalaPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- RNA Structure, Functions WebDocument25 pagesRNA Structure, Functions WebEmad ManniPas encore d'évaluation
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- 931 PDF PDFDocument4 pages931 PDF PDFChintamani VeerrajuPas encore d'évaluation
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Finals ReviewerDocument5 pagesFinals ReviewerARIAR, Jyllianne Kyla C.Pas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Major Intermediates in Organophosphate Synthesis (PCL, Pocl, PSCL, and Their Diethyl Esters) Are Anticholinesterase Agents Directly or On ActivationDocument7 pagesMajor Intermediates in Organophosphate Synthesis (PCL, Pocl, PSCL, and Their Diethyl Esters) Are Anticholinesterase Agents Directly or On ActivationYancy JuanPas encore d'évaluation
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- NMR Spectros PDFDocument14 pagesNMR Spectros PDFAnonymous XX9Om322lPas encore d'évaluation
- Hemodialysis Medical Supply and MedicationDocument10 pagesHemodialysis Medical Supply and Medicationsiuagan.jayveePas encore d'évaluation
- Urea UV Freeze DriedDocument1 pageUrea UV Freeze DriedJanos ImrePas encore d'évaluation
- Ajax Disinfectant CleanserDocument11 pagesAjax Disinfectant CleanserMateusPauloPas encore d'évaluation
- Nta Abhyas Test-65 CDocument5 pagesNta Abhyas Test-65 CMIITY EDUPas encore d'évaluation
- Heat Capacity Lab ReportDocument8 pagesHeat Capacity Lab ReportLiHong Khaw100% (1)
- Minimum VentilationDocument4 pagesMinimum VentilationNathan Smith100% (1)
- Conductivity Theory and PracticeDocument50 pagesConductivity Theory and Practiceতানভীর নূরPas encore d'évaluation
- Embuild BrochureDocument38 pagesEmbuild BrochureKawish TamourPas encore d'évaluation
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Bs en 357 - 2004 Glass-Frp ClassDocument16 pagesBs en 357 - 2004 Glass-Frp ClassKwong chi hoPas encore d'évaluation
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)