Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- G - AbdominalDocument9 pagesG - AbdominalGrore Dagariolem VasiuzereliuPas encore d'évaluation
- Gluten sensitivity may affect the nervous systemDocument5 pagesGluten sensitivity may affect the nervous systemGrore Dagariolem VasiuzereliuPas encore d'évaluation
- Analytic Geometry Formulas PDFDocument4 pagesAnalytic Geometry Formulas PDFKaranbir RandhawaPas encore d'évaluation
- Formulas & Rules for Limits, Derivatives & Higher Order DerivativesDocument2 pagesFormulas & Rules for Limits, Derivatives & Higher Order DerivativesSwapnil GuptaPas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Healthy FoodDocument4 pagesHealthy FoodHector CachoPas encore d'évaluation
- BIOCHEMISTRY CARBOHYDRATESDocument100 pagesBIOCHEMISTRY CARBOHYDRATESJiezl Abellano AfinidadPas encore d'évaluation
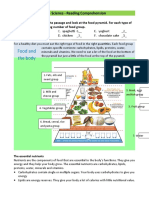
- Food Pyramid Word WorksheetDocument2 pagesFood Pyramid Word WorksheetAnabelPas encore d'évaluation
- Junk Food's Harmful Effects and Healthy SolutionsDocument18 pagesJunk Food's Harmful Effects and Healthy SolutionsMarcela CoroleaPas encore d'évaluation
- Food Calorie ChartDocument23 pagesFood Calorie ChartAshutosh SharmaPas encore d'évaluation
- Subjective Global Assessment Form: Medical HistoryDocument2 pagesSubjective Global Assessment Form: Medical Historynadia susiyanaPas encore d'évaluation
- List of List WomenDocument15 pagesList of List Womencharanmann9165Pas encore d'évaluation
- Risk For Fluid ImbalanceDocument8 pagesRisk For Fluid Imbalanceapi-277522722100% (1)
- Addressing The Gaps in Nutritional Care Before and During PregnancyDocument12 pagesAddressing The Gaps in Nutritional Care Before and During PregnancyBushra KainaatPas encore d'évaluation
- Fats and OilsDocument30 pagesFats and OilsProtec EnergyPas encore d'évaluation
- Ascorbate The Science of Vitamin CDocument272 pagesAscorbate The Science of Vitamin CLuc LiebecqPas encore d'évaluation
- Final VeganDocument11 pagesFinal Veganapi-314696134Pas encore d'évaluation
- Protein: Issa Guide ToDocument11 pagesProtein: Issa Guide ToScooby Doo100% (1)
- Swot and Pestle Analysis of SubwayDocument30 pagesSwot and Pestle Analysis of Subwayhira waqas14100% (2)
- Full Download Test Bank For Williams Basic Nutrition and Diet Therapy 15th Edition by Nix PDF Full ChapterDocument36 pagesFull Download Test Bank For Williams Basic Nutrition and Diet Therapy 15th Edition by Nix PDF Full Chaptergladdenbugler.uy6kz100% (19)
- Dengue Discharge PlanDocument1 pageDengue Discharge PlanChris Denver BancalePas encore d'évaluation
- John K. Mathai, Yanhong Liu and Hans H. SteinDocument10 pagesJohn K. Mathai, Yanhong Liu and Hans H. SteinDébora Giaretta ZattaPas encore d'évaluation
- Goals and ObjectivesDocument5 pagesGoals and ObjectivesAnjela RafiquePas encore d'évaluation
- Natural Ramadan Fat Loss PDFDocument4 pagesNatural Ramadan Fat Loss PDFAhmed KabeerPas encore d'évaluation
- 3 Fitness, Wellness, Stress ManagementDocument43 pages3 Fitness, Wellness, Stress ManagementdaghmouaPas encore d'évaluation
- Color Food PyramidDocument1 pageColor Food PyramidChelsea KranzPas encore d'évaluation
- Anatomy ProjectDocument9 pagesAnatomy Projectapi-391807326Pas encore d'évaluation
- Test I. Calories: Activity No. 6.3Document3 pagesTest I. Calories: Activity No. 6.3Roselie Mae GarciaPas encore d'évaluation
- The Peter Attia Driving framework, vitamin supplementation, antioxidantsDocument21 pagesThe Peter Attia Driving framework, vitamin supplementation, antioxidantsHarryPas encore d'évaluation
- Lab Report For MonossacharideDocument15 pagesLab Report For MonossacharideSay Cheez100% (1)
- Parents Perceptionin School Based Feeding ProgramDocument18 pagesParents Perceptionin School Based Feeding ProgramAiza ConchadaPas encore d'évaluation
- The Shredding Tips Guide PDFDocument33 pagesThe Shredding Tips Guide PDFIzzue RiderPas encore d'évaluation
- Food Chemistry (Cheese) FullDocument11 pagesFood Chemistry (Cheese) FullAlia CameliaPas encore d'évaluation
- Bal DietDocument18 pagesBal DietamberPas encore d'évaluation
- Exchange ListDocument16 pagesExchange ListSaira JabeenPas encore d'évaluation